#1
While as preventive cardiologist we all organize information from imaging and biomarkers in a debate with my dear friend @CBallantyneMD , asked tough Q what would I choose if I had one option?
The answer is clear and maybe not debatable anymore
@ASPCardio @Heart_SCCT
While as preventive cardiologist we all organize information from imaging and biomarkers in a debate with my dear friend @CBallantyneMD , asked tough Q what would I choose if I had one option?
The answer is clear and maybe not debatable anymore
@ASPCardio @Heart_SCCT

# 2 What ur risk? remains the foundational strategy in preventive cardiology and in this pursuit we continue to rely on risk factors and a growing list of biomarkers
@ASPCardio @CBallantyneMD @DrMarthaGulati
@ASPCardio @CBallantyneMD @DrMarthaGulati

# 3
And the goal is worthy as the ACCURATE identifying those at higher but also at low risk is critical for treating the right patient at the right time with the right intervention, societal resource allocation and informed patient choices
And the goal is worthy as the ACCURATE identifying those at higher but also at low risk is critical for treating the right patient at the right time with the right intervention, societal resource allocation and informed patient choices

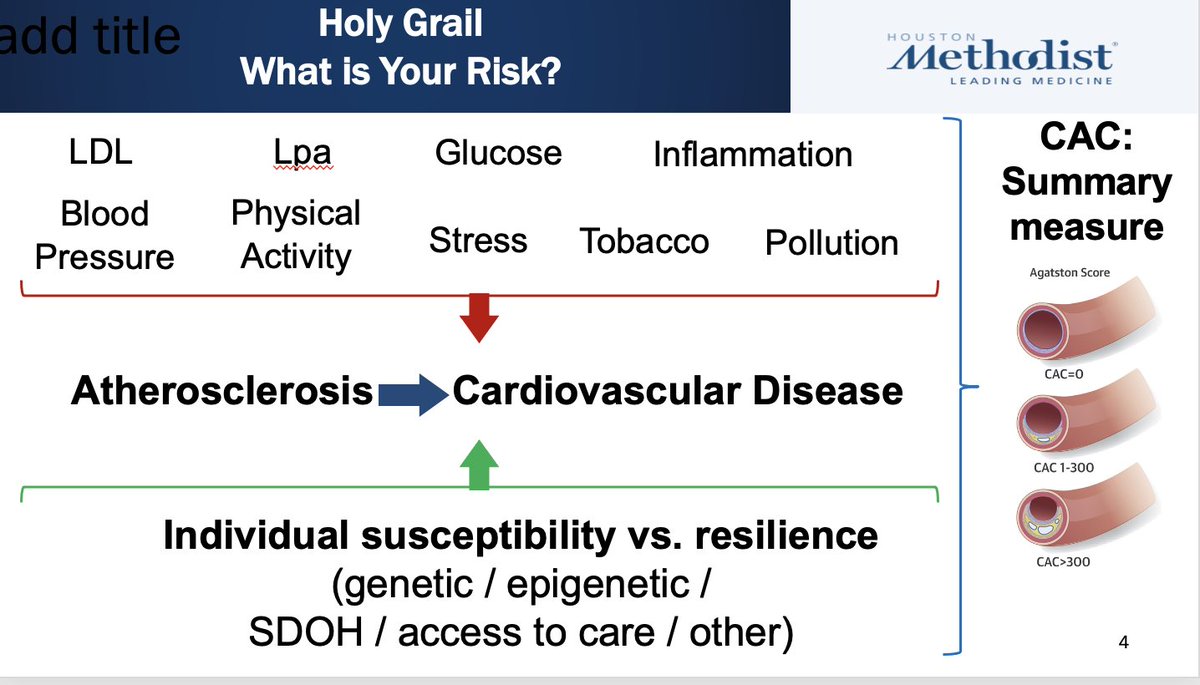
# 4
However, if we believe, atherosclerosis is the main underlying mechanism for CVD clinical complications, then why not focus where the money is only captures the impact of prior exposures as well as accounts for resilience and vulnerability.
However, if we believe, atherosclerosis is the main underlying mechanism for CVD clinical complications, then why not focus where the money is only captures the impact of prior exposures as well as accounts for resilience and vulnerability.
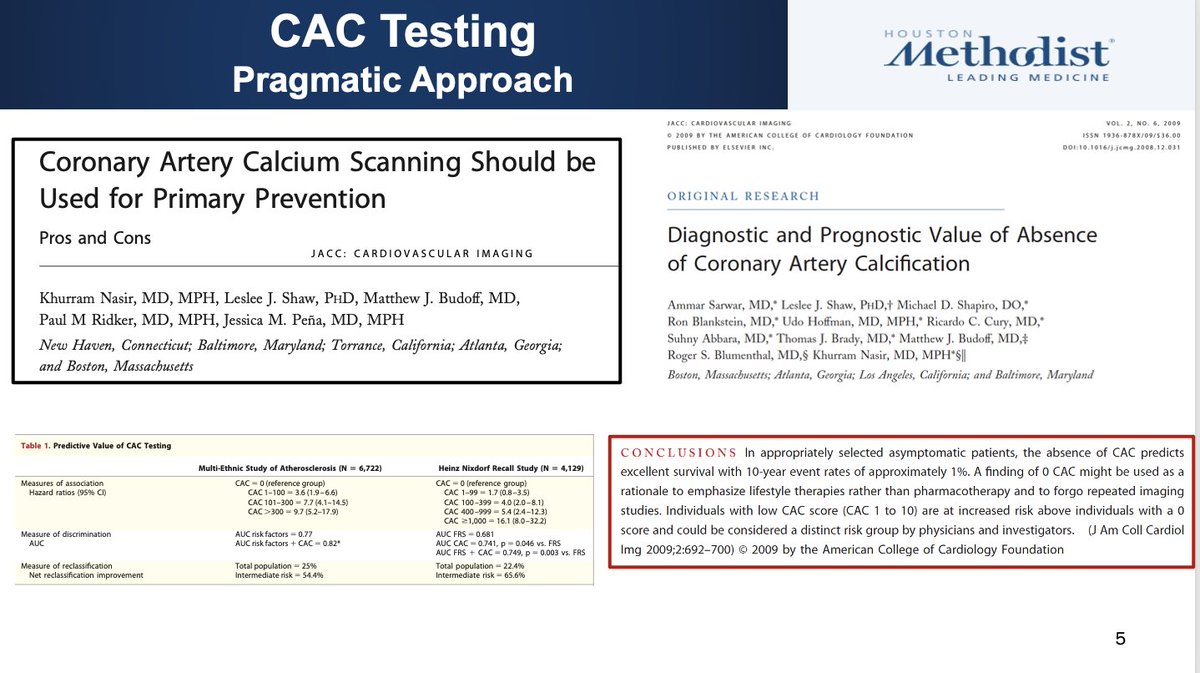
# 5 In this SPACE, clearly CAC is the fleader
s no better marker that predicts those at the highest risk, provides clear discrimination and reclassify the most individuals in a meaningful manner to impact decisions, but also has a feature of most accurately derisking
s no better marker that predicts those at the highest risk, provides clear discrimination and reclassify the most individuals in a meaningful manner to impact decisions, but also has a feature of most accurately derisking
# 6
IRRESPECTIVE OF how u slice and dice the pie of Lipids, the very basic foundational biomarker for CVD risk assessment, in what matters the most is do you have CAC and how much
IRRESPECTIVE OF how u slice and dice the pie of Lipids, the very basic foundational biomarker for CVD risk assessment, in what matters the most is do you have CAC and how much

# 7
While inflammation ALSO remain a “contributor” like Lipids, nearly half of those with elevated hs-CRP have no CAC, you cannot have a more favorable prognosis than what we observe, and truly most of the event happen when there is significant CAC (common sense)
While inflammation ALSO remain a “contributor” like Lipids, nearly half of those with elevated hs-CRP have no CAC, you cannot have a more favorable prognosis than what we observe, and truly most of the event happen when there is significant CAC (common sense)

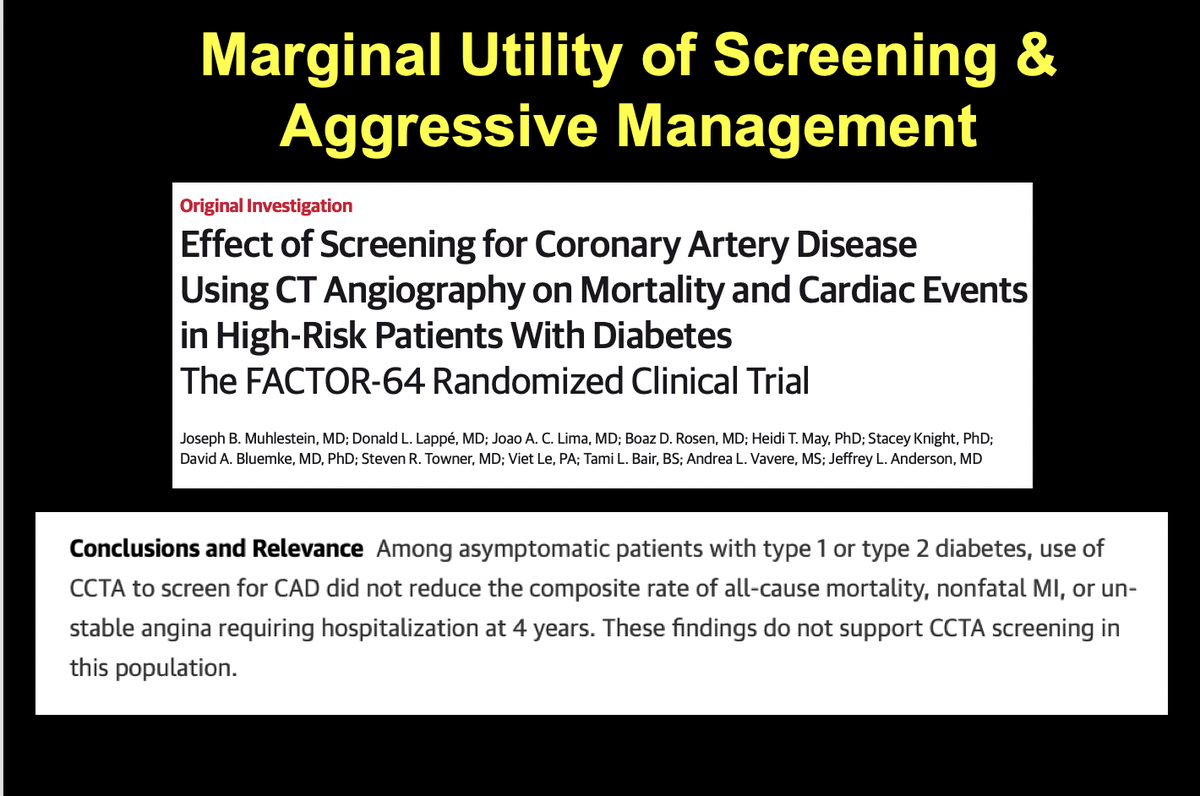
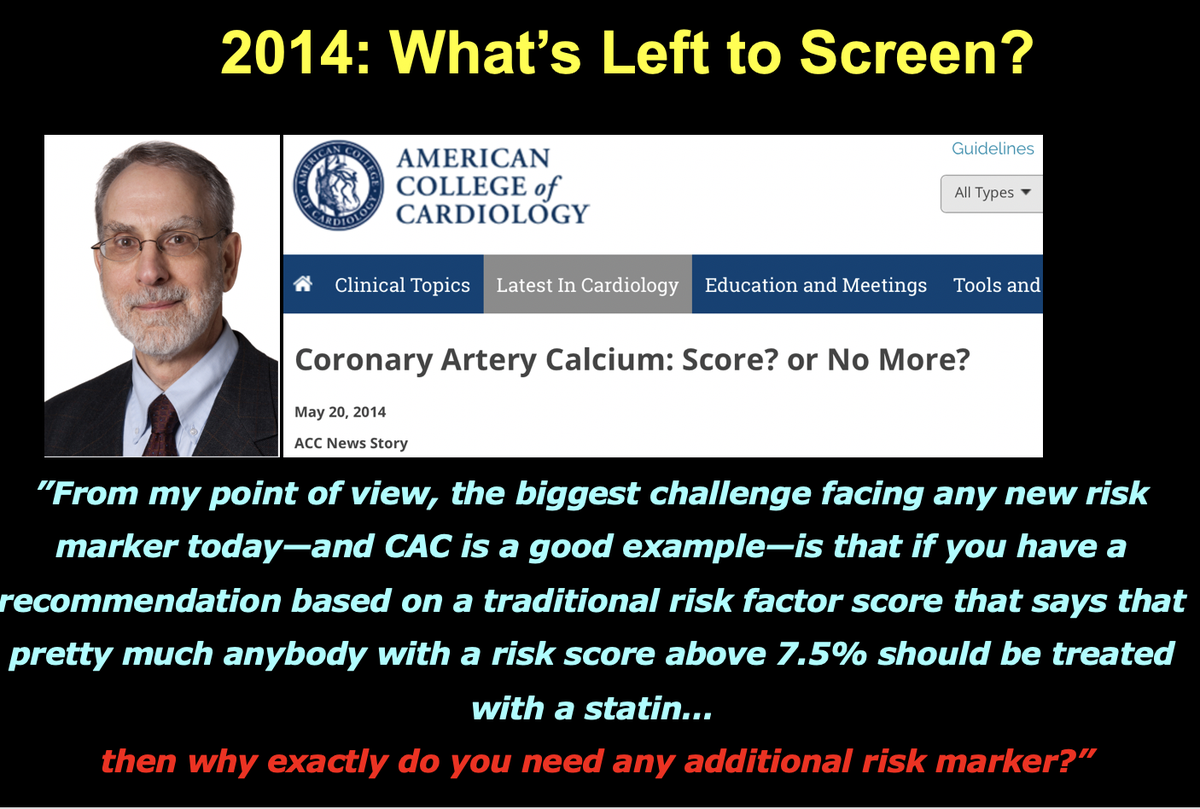
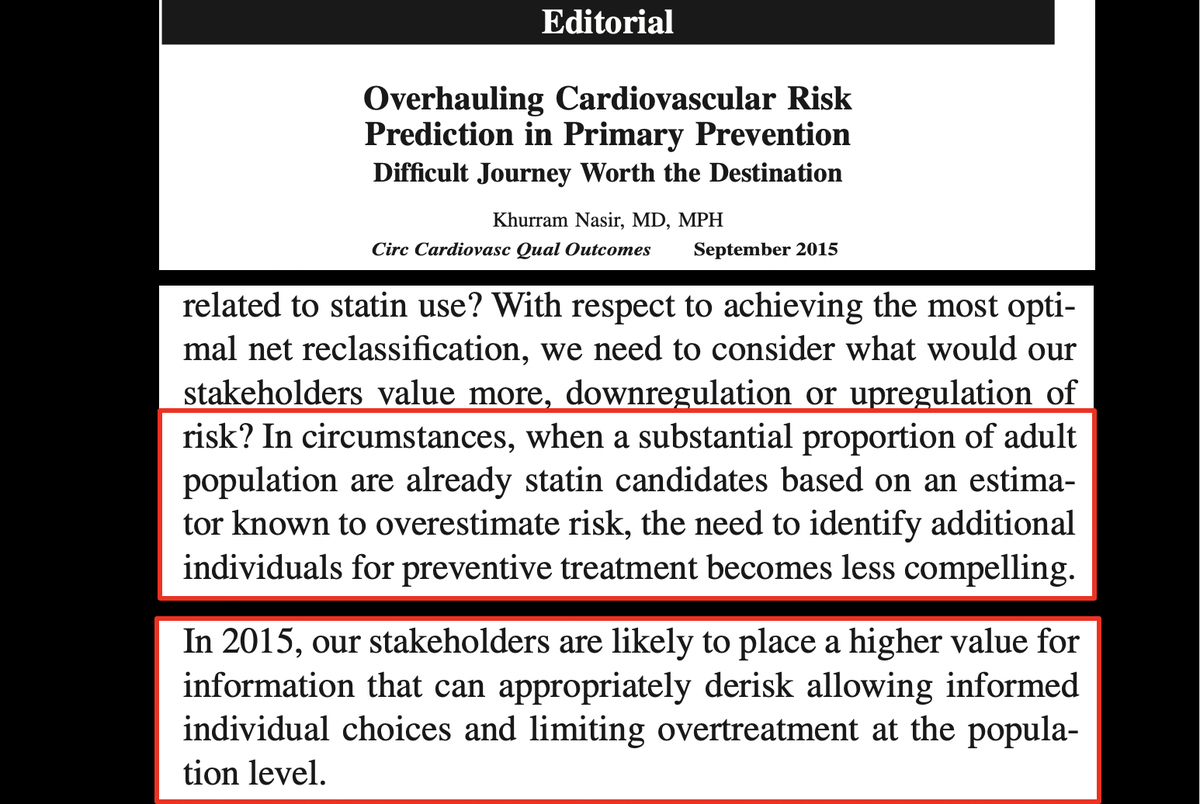
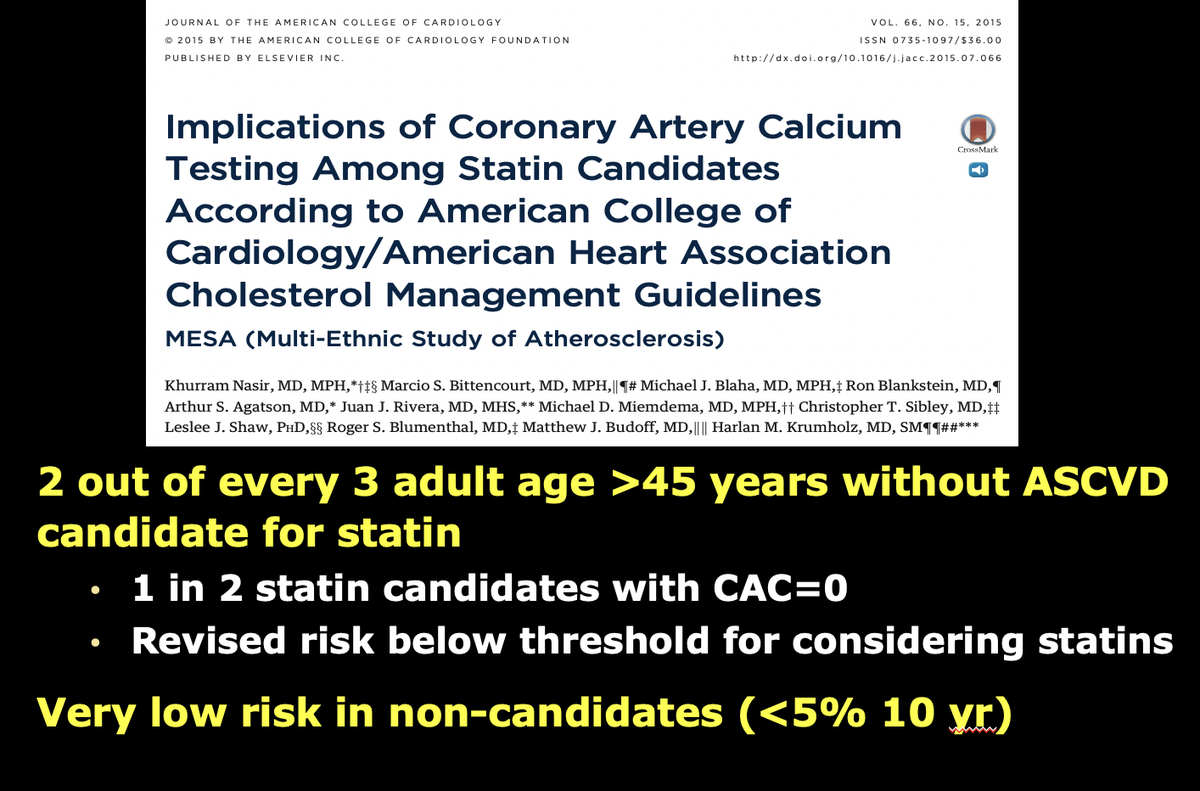
# 8 we clearly showed that CAC based approach overcomes the biomarker based fallacies that can only elevate risk estimates and try to medicate more individuals, CAC actually best to clear out nearly half of individuals who are below the risk threshold for treatment selections

# 9
and not only that now there is data
that for derisking cac zero is peerless,
there is no societal dowsize in guiding statin decisions based on cac
no true benefit of statin with cac zero in 12 yrs fu
and not only that now there is data
that for derisking cac zero is peerless,
there is no societal dowsize in guiding statin decisions based on cac
no true benefit of statin with cac zero in 12 yrs fu

# 10
All of this eventually led the conservative guideline committee to acknowledge undeniable evidence on role of cac and importance of zeor that upgraded use of CAC testing as rec IIA, as a SDM and for the first time that even with abnormal biomarkers for flexibility.
All of this eventually led the conservative guideline committee to acknowledge undeniable evidence on role of cac and importance of zeor that upgraded use of CAC testing as rec IIA, as a SDM and for the first time that even with abnormal biomarkers for flexibility.


# 11
while i am excited about lpa and growing list of ref , but again we see the same pattern of no increased risk with cac zero and mainly explained with higher cac burden, forcing many to question why bother for biomarkers based risk enhancers
while i am excited about lpa and growing list of ref , but again we see the same pattern of no increased risk with cac zero and mainly explained with higher cac burden, forcing many to question why bother for biomarkers based risk enhancers

# 12 also in severe hyperlipidemia no further risk stratification?
13 yr data from mesa suggest nearly 1/3rd of individuals with ldl>190 have power of zero and a 3% 13 yr event rate
another hurdle allowing for a preciosr approach overcome another biomarker based fallacy
13 yr data from mesa suggest nearly 1/3rd of individuals with ldl>190 have power of zero and a 3% 13 yr event rate
another hurdle allowing for a preciosr approach overcome another biomarker based fallacy

# 13
In end choice is yours
Keep doing the same thing or move on with emerging technology
Also CAC helps precisely ensure there is no one size fit all
In end choice is yours
Keep doing the same thing or move on with emerging technology
Also CAC helps precisely ensure there is no one size fit all


@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh