With 5 days to Chol management guidelines update @AHAMeetings..gentle reminder in @JACCJournals: It’s time to accept the #PowerOfZero.
Hope it’s not too late! @rblument1 @hmkyale @MichaelJBlaha @RonBlankstein @ErinMichos @MBittencourtMD.
Some thoughts👇
onlinejacc.org/content/early/…
Hope it’s not too late! @rblument1 @hmkyale @MichaelJBlaha @RonBlankstein @ErinMichos @MBittencourtMD.
Some thoughts👇
onlinejacc.org/content/early/…
#1 Going back to early 2000’s when many showed RF-based approach fell short for individual patient management decisions... aspirations for CAC ‘screening’ gained momentum, though progress stalled due to lack of RCT & waiting for prospective cohorts to confirm prognostication

#3, while hard to rationalize @NIH aversion to fund much needed RCT, sig progress with MESA & HNR confirmed CAC risk stratification capacity->In 2010 Class IIa rec for ‘screen-detect disease-treat’. At that time many hoped next guidelines update wud strengthen CAC screening recs
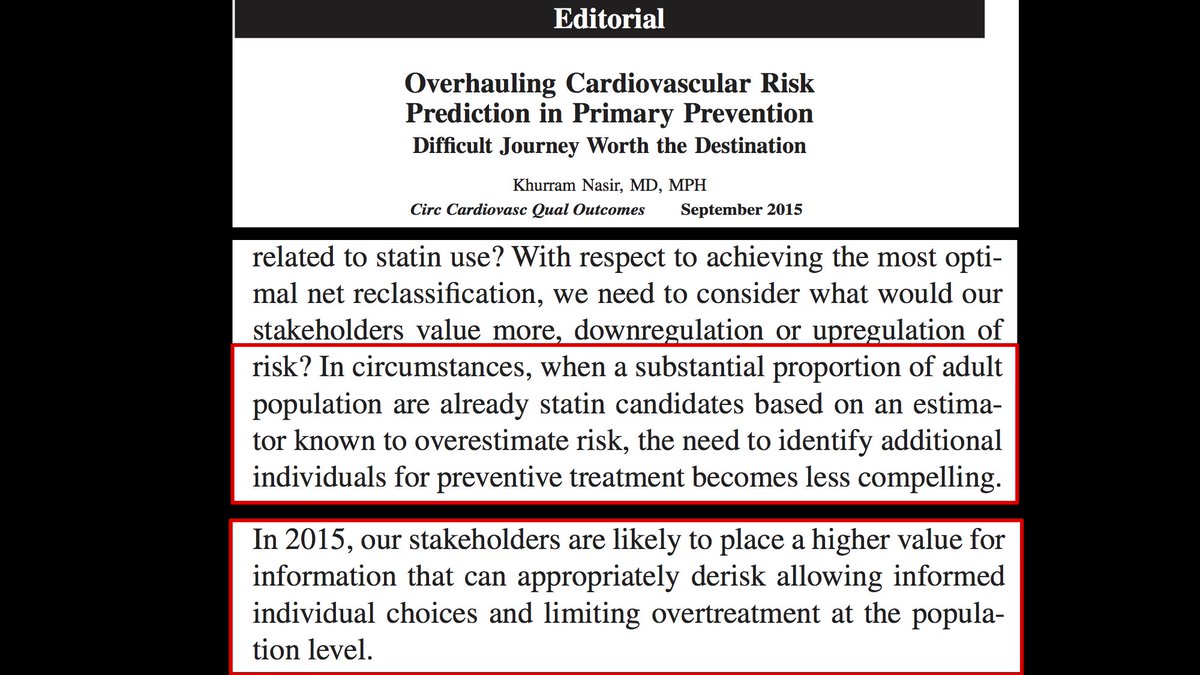
#4, On the other hand, amid criticism of underestimating risk, the 2013 Chol management guidelines rather choose to broaden the scope of statin eligibility. With more than half statin candidates & need for screening less compelling, unfortunately CAC downgraded to IIB rec.

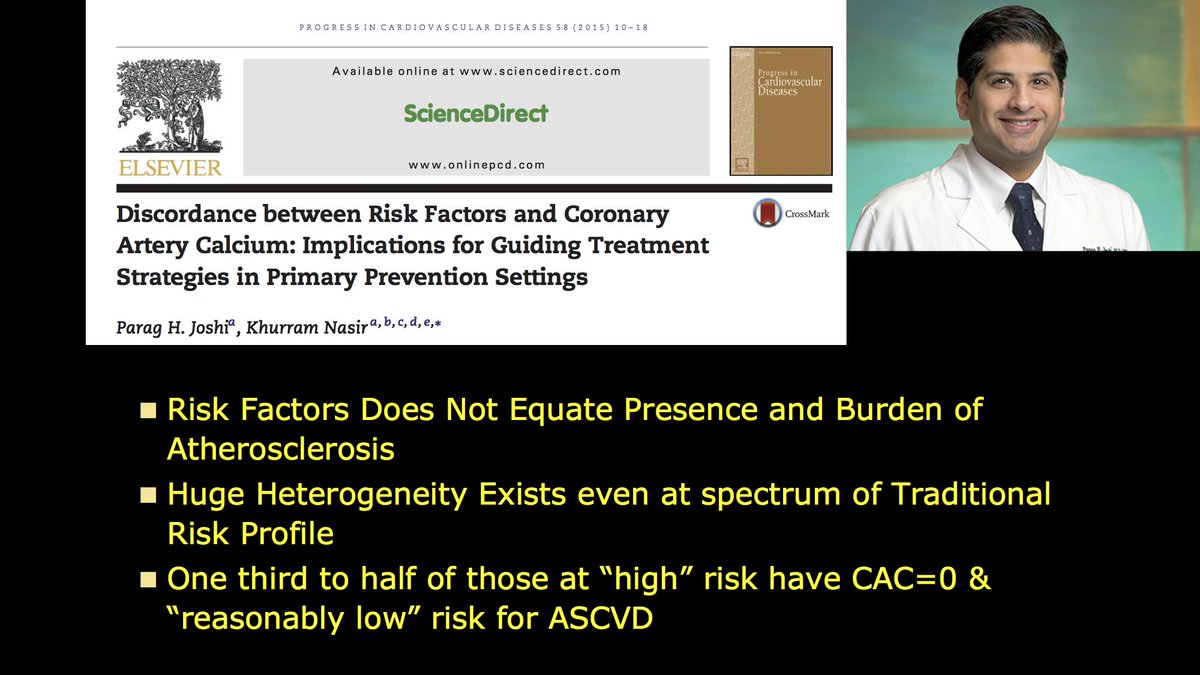
#5 This change did made me pause to question value of screening paradigm. In 2015 i argued that with possible risk of mass statinization, stakeholders likely to appreciate derisking & CAC testing value can be unlocked with focus on ‘absence’ vs ‘presence’ of disease


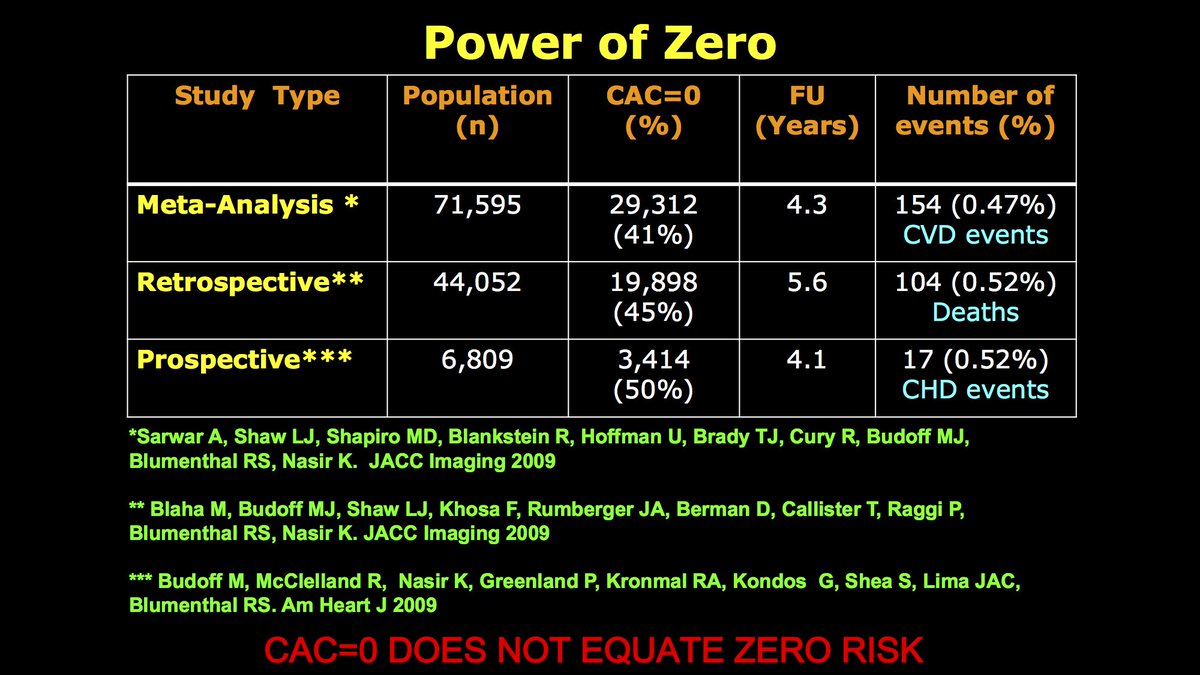
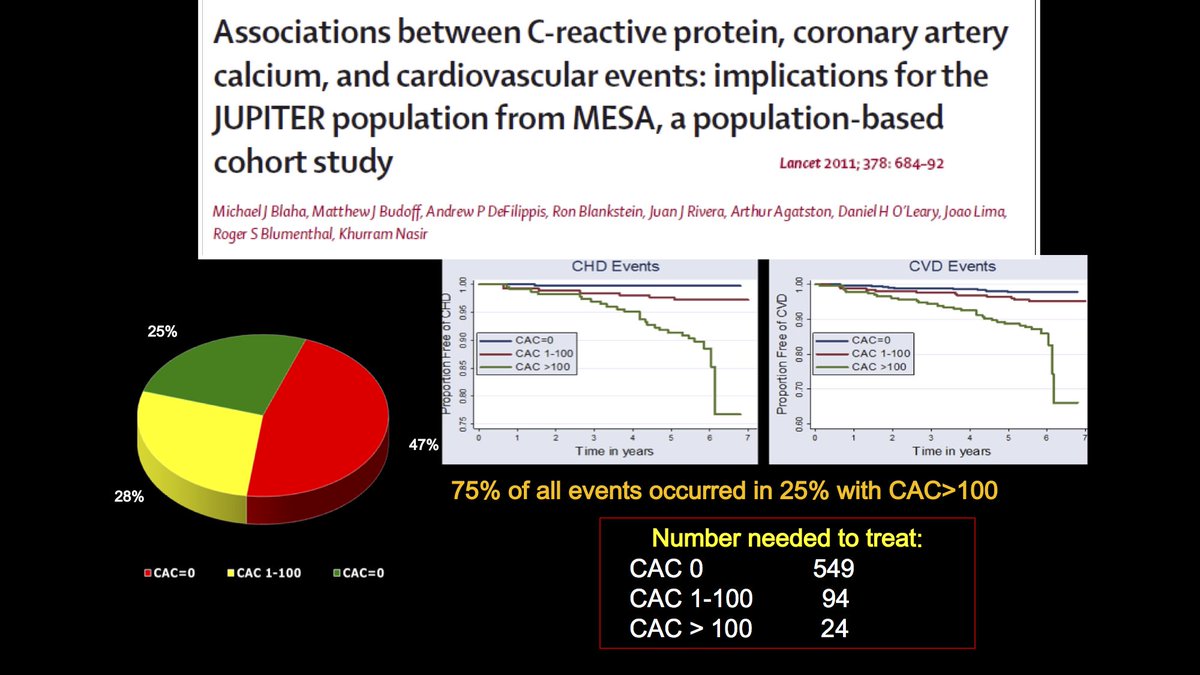
#6 this notion was based on #ThePowerOfZero, introduced by our group in 2009, in 2015 we showed how CAC=0 can inform statin decisions within context of current guidelines. Focus on 5-20%, little value at extreme risk-> eventually informed 2017 @Heart_SCCT CAC consensus statement
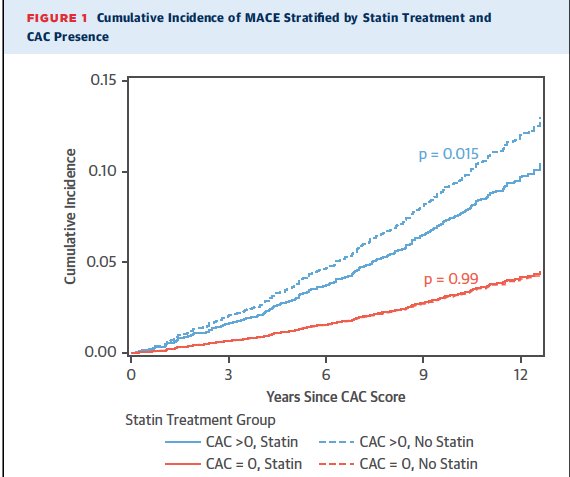
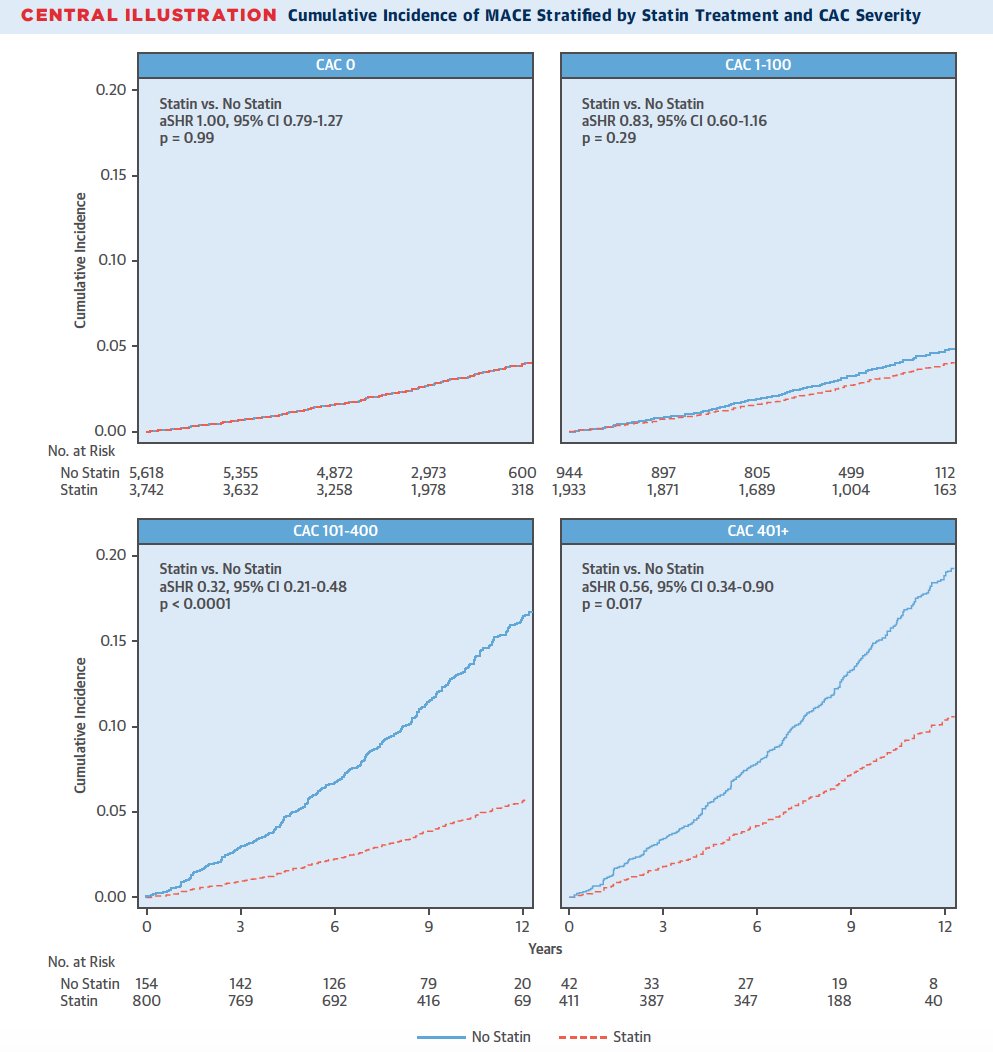
#7 despite this, in 2018 many remain on fence reg #ThePowerofZero. Today this paper by Todd Villinness group @jaccjournals show a) Among CAC=0 little benefit with statin over 10 yrs, b) greater benefit with higher CAC, NNT=12 to prevent 1 event if CAC>100 onlinejacc.org/content/early/…
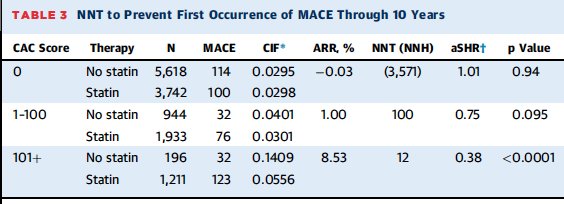
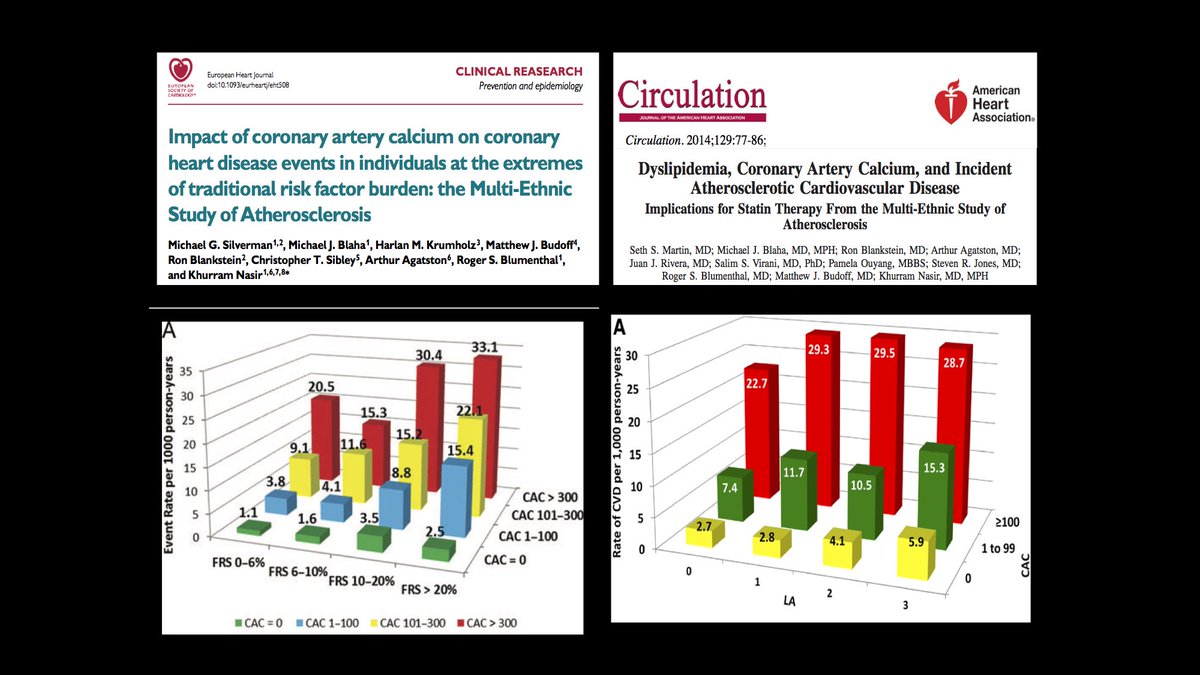
#8 It also confirmed our prior paper proposal that CAC less valuable at risk extremes, few in <5% risk had CAC>100 to impart benefit, CAC=0 among >20% benefited with statin. By focusing on 5-20% risk range via CAC=0/CAC>0 pop. dichotomized in who will & not benefit from statin

#9 Now what? I think chol managements guidelines @AHAMeetings have an excellent opportunity to make amends. Can’t hide anymore behind dogmatic pretense ‘lack of RCT’, enough data generated in 5 yrs for CAC to be afforded IIA rec as a ‘decision tool’ in intermediate risk patients
#10 In short, CAC's has remarkably resurrected by transitioning its initial proposed role as screening tool to decision-aid, eloquently described by @hmkyale “This test might tell you if you don't need a statin”. Now time for guidelines to muster COURAGE & accept #ThePowerof Zero