Hi #medtwitter #neurotwitter #medstudenttwitter #meded #FOAMed
It's been too long since my last #EndNeurophobia #tweetorial. As requested by @sukritibanthiya here is a tweetorial on MUSCLE DISEASE (MYOPATHY)
Let me know what you think and what I should cover next!
It's been too long since my last #EndNeurophobia #tweetorial. As requested by @sukritibanthiya here is a tweetorial on MUSCLE DISEASE (MYOPATHY)
Let me know what you think and what I should cover next!

Classic pattern of weakness in myopathy is PROXIMAL symmetric weakness of the limbs, though there are exceptions.
There should be NO sensory findings (unless there is concurrent neuropathy) and reflexes are often spared until the patient is extremely weak.
There should be NO sensory findings (unless there is concurrent neuropathy) and reflexes are often spared until the patient is extremely weak.
Difficulty rising from a chair (hip girdle musculature), washing hair (shoulder girdle musculature)
CK is often elevated but not always
EMG can demonstrate myopathic pattern (though can be normal eg statin myopathy)
Definitive Dx may require muscle biopsy and/or genetic test
CK is often elevated but not always
EMG can demonstrate myopathic pattern (though can be normal eg statin myopathy)
Definitive Dx may require muscle biopsy and/or genetic test
There are so many causes of myopathy.
I divide into 5 broad categories to consider:
INFLAMMATORY
GENETIC
SECONDARY TO SYSTEMIC DISEASE
TOXIC
INFECTIOUS
I divide into 5 broad categories to consider:
INFLAMMATORY
GENETIC
SECONDARY TO SYSTEMIC DISEASE
TOXIC
INFECTIOUS

INFLAMMATORY:
In med school, I learned 2:
Dermatomyositis (DM) & Polymyositis (PM)
Both with proximal weakness
Dermato with skin findings (mechanic hands, Gottron papules, V sign on neck, shawl sign on back heliotrope rash of eyelids), a/w malignancy
Different findings on path
In med school, I learned 2:
Dermatomyositis (DM) & Polymyositis (PM)
Both with proximal weakness
Dermato with skin findings (mechanic hands, Gottron papules, V sign on neck, shawl sign on back heliotrope rash of eyelids), a/w malignancy
Different findings on path
In residency, I learned:
Inclusion body myositis (IBM): weakness long finger flexors, quads, dorsiflexion; dysphagia, asymmetry may occur; more common in men>50), may be a/w T cell large granular lymphocytic leukemia.
Immune-mediated necrotizing: may/may not be statin-induced
Inclusion body myositis (IBM): weakness long finger flexors, quads, dorsiflexion; dysphagia, asymmetry may occur; more common in men>50), may be a/w T cell large granular lymphocytic leukemia.
Immune-mediated necrotizing: may/may not be statin-induced
This keeps getting more complicated as more antibodies are discovered that correlate w/particular syndromes:
DM: Anti-MDA-5, Mi-2, SAE, NXP-2, TIF-1 (last 2 a/w ⬆️ risk malignancy)
IBM: anti-cytoplasmic 5’-nucleotidase 1A
Immune-mediated necr: anti-HMG CoA reductase, anti-SRP
DM: Anti-MDA-5, Mi-2, SAE, NXP-2, TIF-1 (last 2 a/w ⬆️ risk malignancy)
IBM: anti-cytoplasmic 5’-nucleotidase 1A
Immune-mediated necr: anti-HMG CoA reductase, anti-SRP
Anti-synthetase syndrome: anti-Jo-1, PL-7, PL-12 a/w myositis, mechanic’s hands, Raynaud phenomenon, arthritis, and interstitial lung disease
Colleagues tell me they’re not even sure PM exists as a unique entity anymore…
Most inflam myop respond to immunomod; IBM doesn't
Colleagues tell me they’re not even sure PM exists as a unique entity anymore…
Most inflam myop respond to immunomod; IBM doesn't
GENETIC
I divide these into:
DYSTROPHIES: mutations in muscle proteins
METABOLIC: mutations in metabolic pathways
MITOCHONDRIAL: mutations in mitochondrial genes
PERIODIC PARALYSES: mutations in ion channels
I divide these into:
DYSTROPHIES: mutations in muscle proteins
METABOLIC: mutations in metabolic pathways
MITOCHONDRIAL: mutations in mitochondrial genes
PERIODIC PARALYSES: mutations in ion channels
DYSTROPHIES
Duchenne, Becker, Fascioscapulohumeral, Limb-Girdle, Oculopharyngeal, Myotonic, Emery-Dreifuss, Distal dystrophies...
Names mostly explain sites of weakness
Many have cardiac involvement
E-D has prominent contractures
Duchenne, Becker, Fascioscapulohumeral, Limb-Girdle, Oculopharyngeal, Myotonic, Emery-Dreifuss, Distal dystrophies...
Names mostly explain sites of weakness
Many have cardiac involvement
E-D has prominent contractures

Distal dystrophies
Rare and break “myopathy = proximal” rule. They present almost all with DORSIFLEXION weakness, though Miyoshi affects plantarflexion, and Welander also affects the hands.
I’ve never seen any of these outside of conference presentations and text books.
Rare and break “myopathy = proximal” rule. They present almost all with DORSIFLEXION weakness, though Miyoshi affects plantarflexion, and Welander also affects the hands.
I’ve never seen any of these outside of conference presentations and text books.
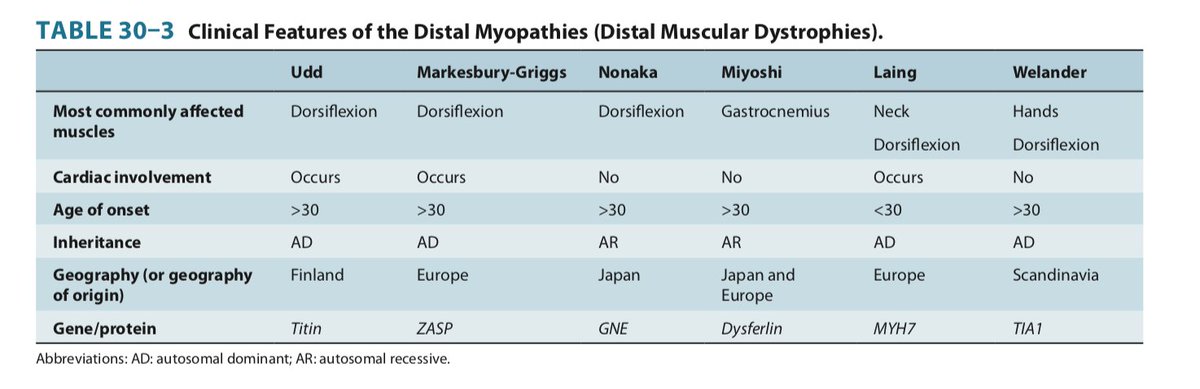
Want to look smart and rattle these off @ a conference?Here’s a mnemonic:
U
M
L M N + W
Of course they don’t affect UMN or LMN, but just mnemonic. MiyOshi affects gastrOc, LaiNg the neck, WelANDer the hAND.
Thought these would be on the boards. They weren’t.
U
M
L M N + W
Of course they don’t affect UMN or LMN, but just mnemonic. MiyOshi affects gastrOc, LaiNg the neck, WelANDer the hAND.
Thought these would be on the boards. They weren’t.
Metabolic myopathies
The one for adult neurologists to know is adult-onset Pompe disease (acid maltase deficiency) as it may not have the exercise-induced symptoms of the others and present simply w/proximal weakness–and it’s treatable w/enzyme replacement!
The one for adult neurologists to know is adult-onset Pompe disease (acid maltase deficiency) as it may not have the exercise-induced symptoms of the others and present simply w/proximal weakness–and it’s treatable w/enzyme replacement!

Mitochondrial myopathy:
Often other features of multi-system disease.
If you see epilepsy + myopathy, think mitochondrial, e.g., MERRF (myoclonic epilepsy w/ragged red fibers), mutation in A8344G (I remember the RR - 44 for the boards)
Often other features of multi-system disease.
If you see epilepsy + myopathy, think mitochondrial, e.g., MERRF (myoclonic epilepsy w/ragged red fibers), mutation in A8344G (I remember the RR - 44 for the boards)
PERIODIC PARALYSES
I’ve never seen these in real life. But would be a diagnosis to consider if a patient becomes paralyzed after a high carb meal (hypoK periodic paralysis) or fasting/exercise (hyperK periodic paralysis) and has abnormal K on BMP
I’ve never seen these in real life. But would be a diagnosis to consider if a patient becomes paralyzed after a high carb meal (hypoK periodic paralysis) or fasting/exercise (hyperK periodic paralysis) and has abnormal K on BMP

SYSTEMIC DISEASES
Rheumatologic disease (lupus, systemic sclerosis): called overlap myopathy (anti-Ku, anti-PMScl, and anti-U1 RNP may be seen)
Endocrine (hypo/hyperthyroid, Cushing's (intrinsic or iatrogenic)
Critical illness myopathy
Rheumatologic disease (lupus, systemic sclerosis): called overlap myopathy (anti-Ku, anti-PMScl, and anti-U1 RNP may be seen)
Endocrine (hypo/hyperthyroid, Cushing's (intrinsic or iatrogenic)
Critical illness myopathy
INFECTIONS
Viral (HIV)
Parasitic: trichinosis (affecting face/eye muscles), toxo, cysticercosis (usually asymptomatic)
Bacterial: muscle abscess/pyomyositis.
Viral (HIV)
Parasitic: trichinosis (affecting face/eye muscles), toxo, cysticercosis (usually asymptomatic)
Bacterial: muscle abscess/pyomyositis.
MEDICATIONS
*STATINS*: anything from asymptomatic ⬆️CK to acute necrotizing myopathy. Higher dose, older age, concurrent fibrates increase risk
Immunomodulatory therapies (steroids, chloroquine, colchicine, cyclosporine, tacrolimus)
Checkpoint inhibitors
Amiodarone
Zidovudine
*STATINS*: anything from asymptomatic ⬆️CK to acute necrotizing myopathy. Higher dose, older age, concurrent fibrates increase risk
Immunomodulatory therapies (steroids, chloroquine, colchicine, cyclosporine, tacrolimus)
Checkpoint inhibitors
Amiodarone
Zidovudine
OK, what did I miss @CrystalYeoMDPhD ?
Want more tweetorials?twitter.com/i/events/12671…
#EndNeurophobia 🧠❤️
Source of tables: amazon.com/gp/product/B01…
Want more tweetorials?twitter.com/i/events/12671…
#EndNeurophobia 🧠❤️
Source of tables: amazon.com/gp/product/B01…
• • •
Missing some Tweet in this thread? You can try to
force a refresh