#ESCCongress #ESCGuidelines This is a Long thread on Heart Failure Guidelines published @escardio #EHJ academic.oup.com/eurheartj/adva… LONG BUT EDUCATIONAL! Focus on CHRONIC HF #epeeps #CardioEd @AlexFrogoudaki @mmamas1973 @DrMarthaGulati @purviparwani @Filippatos @EkateriniL @Hragy …/2 

#ESCCongress Firstly, no longer Mid Range, replace by MILDLY REDUCED LV EF. Makes a lot of sense - in fact for some time I thought the previous guidelines referred to ‘mildly reduced’ until @merinopoulos corrected me… otherwise no real change in the nomeculture …/3

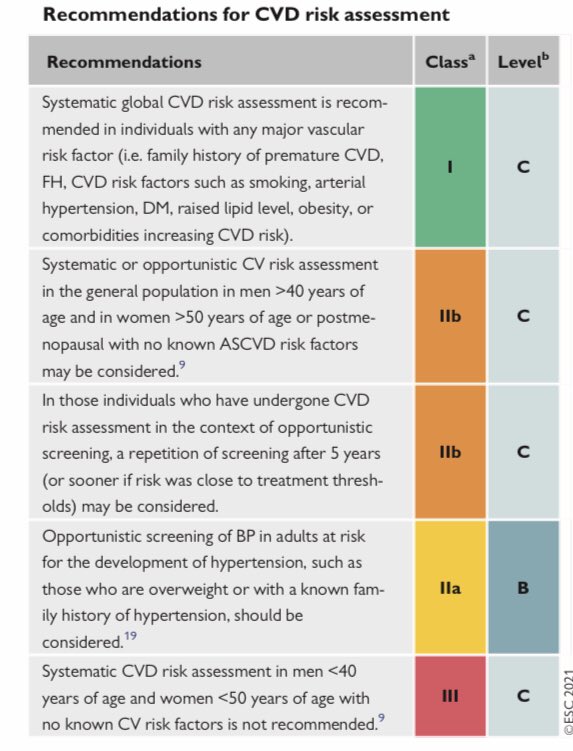
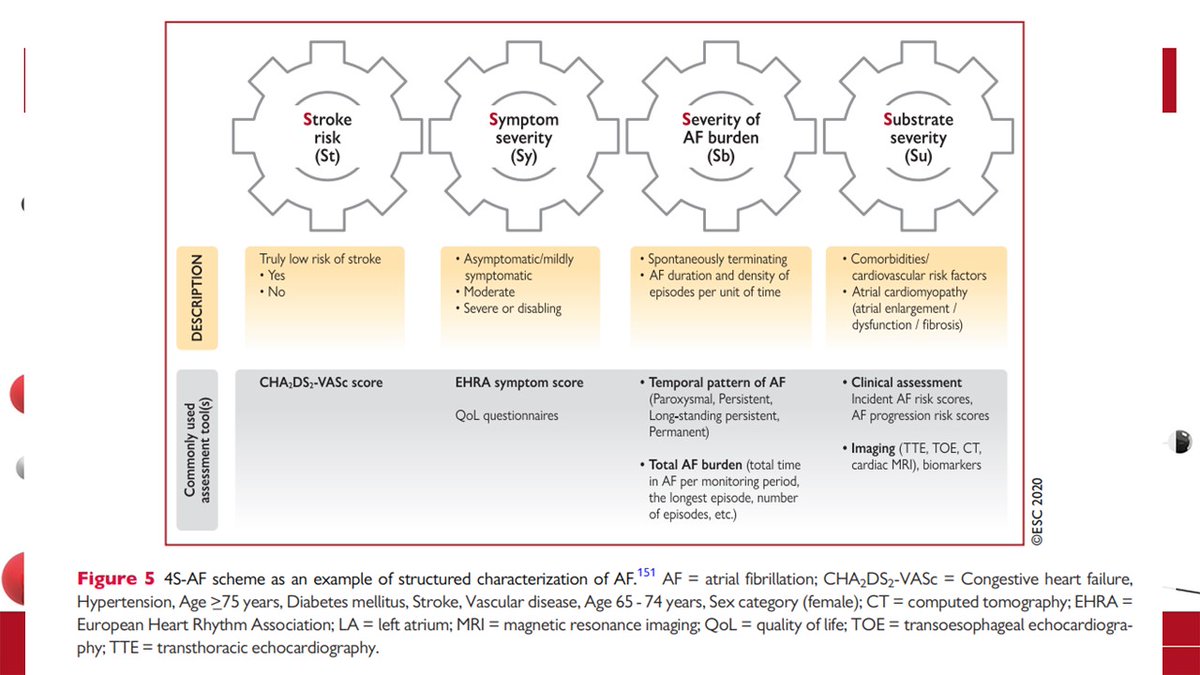
#ESCCongress nice algorithm - assess risk factors… do BNPs (watch the caveats- AF ⬆️ , obesity ⬇️ value so bear this in mind. The #echofirst and classification into Reduced, mildly Reduced and Preserved. @SineadHughes19 @wordfinga @rahatheart1 @HEARTinMagnet @bp_halliday …/4

#ESCCongress symptoms reaffirmed (ok nothing new here) and doses of medication - please STOP THE PRESCRIPTION OF RAMIPRIL 1.25mg! @ShrillaB @MadalinaGarbi @nabeelsheikh99 @pharmabadboy @Johnett72359965 …/5


#ESCCongress & MY FAVOURITE PART. #WhyCMR mainly focused on utilising w poor echo Windows (agree), rule out infiltrative conditions (agree) + to look for LGE in DCM - well here I agree but I think the recommendation could have been stronger here, the evidence is overwhelming …/6

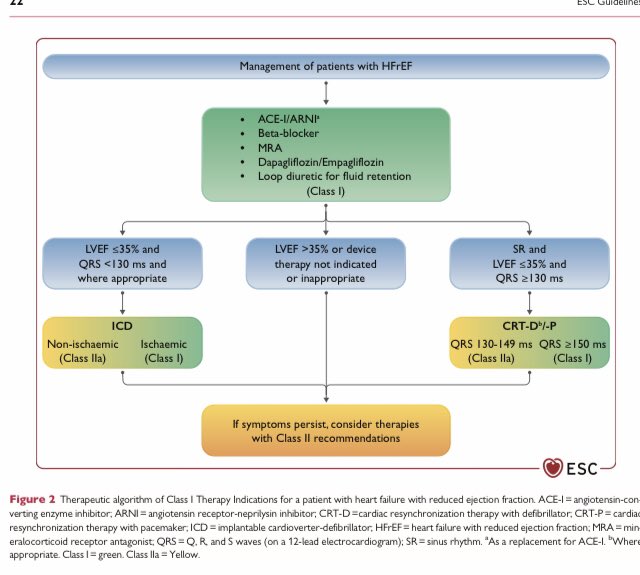
#ESCCongress and a nice info graphic on what each medication 💊 benefits… ACE I/ARNI & Beta blockers & MRA & SGLT2i FOR HFrEF. Again no real change from the recent additions to the guidelines …/7

#ESCCongress on the basis of LVEF and QRS a decision about ICD vs CRT. Am a bit uncomfortable for the IIa for non-ischaemic cardiomyopathy for ICD. We know arrhythmia in NICDM is driven more by mid wall LGE than EF. EF drives heart failure deaths. Time to have included scar …/8
#ESCCongress moving to MILDLY REDUCED LVEF…remember this is anyone with EF 41% upwards. All tablets only given class IIa- I.e ‘can be considered’. I think this could have been a IIa recommendation. And doesn’t include SGLT2i- Emperor-Preserved suggests benefit in this group …/9


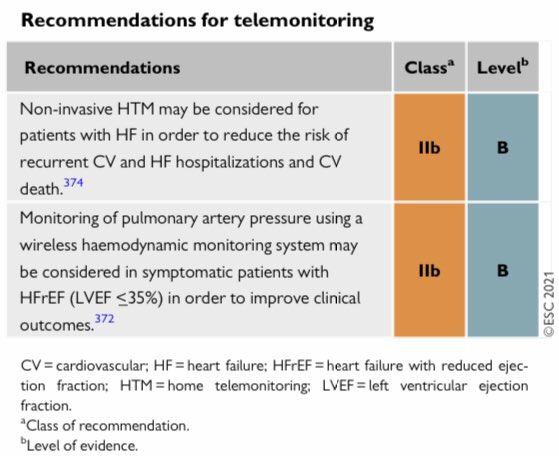
#ESCCongress and the role of rehab following heart failure? A definite YES! Let’s not forget that! Use of TELEMEDICINE- possibly consider. I would say definitely during current times in #covid- as hybrid at least! …/10

#ESCCongress and for advanced heart failure- a nice diagram! But suggest you get your local specialist like @drstephenpettit for specific advice! …/11

So coming to the end- what is the short summary?
1- new name- mildly reduced than mid-range 2- therapy different for each category 3- tablets same as before, SGLT2i in HFrEF 4-remember ICD, CRT- ivabradine if needed …/12
1- new name- mildly reduced than mid-range 2- therapy different for each category 3- tablets same as before, SGLT2i in HFrEF 4-remember ICD, CRT- ivabradine if needed …/12
And last tweet 5- HFmrEF drive to treat same way as HFrEF, lower level evidence. I have to say I enjoyed this guideline, shortish (95 pages) to the point and relatively up to date- although it already needs revisions (Emperor-Preserved for HFmrEF group) Thank u 4 reading. THE END
• • •
Missing some Tweet in this thread? You can try to
force a refresh