
This thread caused quite a stir. Though I can't confirm these numbers (the US doesn't have accessible national data), it's an important idea. If we are indeed all supposed to "get" infected by #SARS2 sooner or later, it would be very useful to know what outcomes we are facing.
1/
1/
https://twitter.com/MCSlab_uiuc/status/1436423893833691138
Once again, I turn to the country that had multiple significant outbreaks, since the beginning collects & now releases in real-time raw data separated by the vaccination status: #Israel.
So, let's compare case fatality rates & case severe hospitalization rates.
2/
So, let's compare case fatality rates & case severe hospitalization rates.
2/
These are #Israel's totals of cases, new severe patients & deaths. I have to stress that Israel tests a lot & includes antigen tests. Their level of healthcare is among the best in the world. And importantly, they reacted swiftly & blunted the impact of both #Alpha & #Delta.
3/
3/
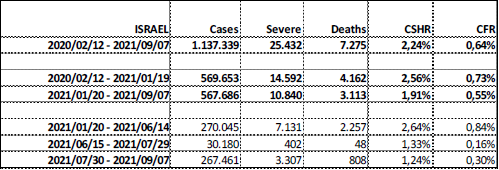
That's why their all-time CFR is so low at 0,64%, or x3 below the world average. Most other countries can only dream of repeating their results.
Next, I divided the numbers before the start of the vaccination campaign & after (data available from Jan 20, 2021).
4/
Next, I divided the numbers before the start of the vaccination campaign & after (data available from Jan 20, 2021).
4/

We can see here vaccination campaigns (both original & booster) additionally helped CFR decrease 0,73% -> 0,55%. Nevertheless, about 28% of severe cases still die.
Subdividing the two main time-frames into shorter intervals is too brief & unfinished for meaningful conclusions.
5/
Subdividing the two main time-frames into shorter intervals is too brief & unfinished for meaningful conclusions.
5/
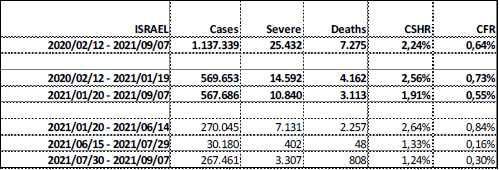
I want to point out Israel enacted a booster campaign while there were 402 new severe cases & only 48 deaths from June 15 to July 29. This remarkable decisiveness is unparalleled in the Western world. Our politicians react only when hospitals & morgues are already overfull.
6/
6/
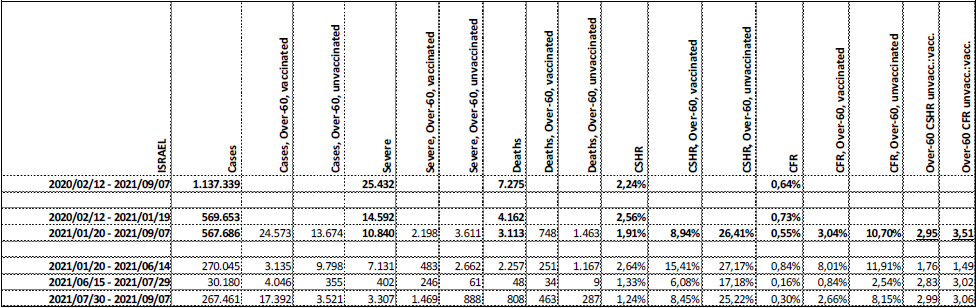
Now I add age subgroups, but I combined vaccinated with or without boosters, while partially vaccinated are not available.
From January 20 until September 7, vaccinated Over-60s have a CFR of 3% vs. 10,7% for the unvaccinated over the same period.
7/
From January 20 until September 7, vaccinated Over-60s have a CFR of 3% vs. 10,7% for the unvaccinated over the same period.
7/

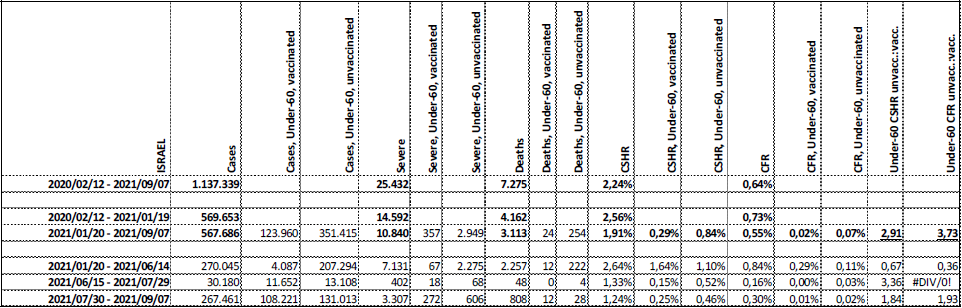
For the Under-60s, in the same period, CFR is incredibly low 0,02% among vaccinated, but 0,07% in unvaccinated.
So, in both the Over-60 & Under-60 subgroups, Israel data shows that the risk of dying after the #SARS2 infection is x3,5 higher for unvaccinated!
8/
So, in both the Over-60 & Under-60 subgroups, Israel data shows that the risk of dying after the #SARS2 infection is x3,5 higher for unvaccinated!
8/

Vaccination also further amplified #SARS2 notorious disproportionality of outcomes. The difference in risk of the fatal outcome between old & young has risen from x150 to x500 when comparing vaccinated Under-60 person to an unvaccinated Over-60.
9/
9/


Case severe hospitalization risk reduction after vaccination is also significant, almost x3 in both age groups. But, if people get into a severe condition, the benefits of vaccines diminish (34% vacc. vs. 40% unvacc.) & age matters much more again (6,7% vacc. & 8,6% unvacc.).
10/
10/

Finally, due to extreme disproportionality of outcomes & vaccination levels, it can be misleading to look at the whole population. Taken all groups together, the general population shows no benefit in CFR. But, as I explained multiple times, it's just a mathematical quirk.
11/11
11/11



• • •
Missing some Tweet in this thread? You can try to
force a refresh






