
1/ 📢📢#tweetorial alert# 📢📢
#nephtwitter #medtwitter
Poll: What are the complications of Renal biopsy?🔫
#nephtwitter #medtwitter
Poll: What are the complications of Renal biopsy?🔫
2/ Bleeding can occur at 3 sites:
🚩Into the collecting system➡️ microscopic or gross hematuria ➡️ureteral obstruction
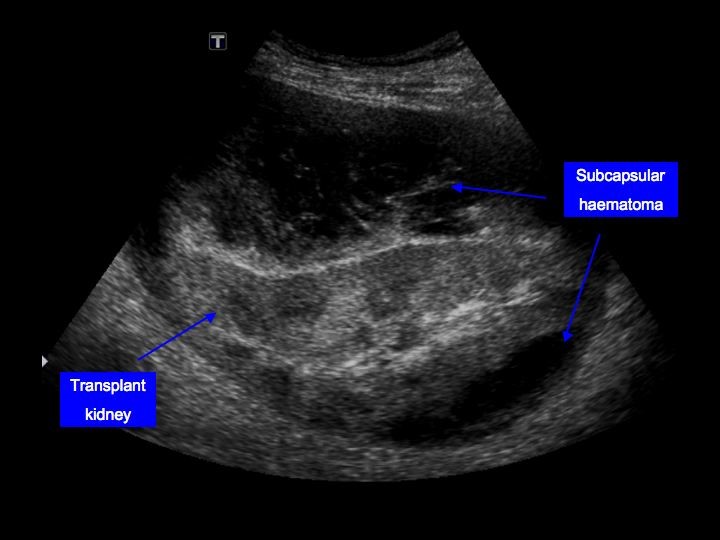
🚩Underneath the renal capsule ➡️ pressure tamponade & pain
🚩Into the perinephric space ➡️ hematoma formation
pubmed.ncbi.nlm.nih.gov/10846435/
🚩Into the collecting system➡️ microscopic or gross hematuria ➡️ureteral obstruction
🚩Underneath the renal capsule ➡️ pressure tamponade & pain
🚩Into the perinephric space ➡️ hematoma formation
pubmed.ncbi.nlm.nih.gov/10846435/


3/ Rarely, severe bleeding may occur due to puncture of : 🩸
📌renal artery,
📌aorta
📌venous collaterals ( in renal vein thrombosis)
📌renal artery,
📌aorta
📌venous collaterals ( in renal vein thrombosis)
4/ What are risk factors for bleeding 🩸⁉️
1.HTN,
2. ⬇️GFR,
3.anemia,
4.older age, 👩🦼
5.use of a larger (14 gauge) biopsy needle🔫
1.HTN,
2. ⬇️GFR,
3.anemia,
4.older age, 👩🦼
5.use of a larger (14 gauge) biopsy needle🔫
5/Poll: Which is the most common complication of renal biopsy?🔫🩸
6/ Incidence of bleeding complications:
📌Pain at biopsy site–4.3%
📌Transient macroscopic hematuria–3.5%
📌Perinephric hematomas–11%
📌Requirement for transfusion–1.6%
📌Requirement for intervention–0.3%
📌Requirement for nephrectomy–0.01%
📌Death–0.06%
pubmed.ncbi.nlm.nih.gov/33060160/
📌Pain at biopsy site–4.3%
📌Transient macroscopic hematuria–3.5%
📌Perinephric hematomas–11%
📌Requirement for transfusion–1.6%
📌Requirement for intervention–0.3%
📌Requirement for nephrectomy–0.01%
📌Death–0.06%
pubmed.ncbi.nlm.nih.gov/33060160/
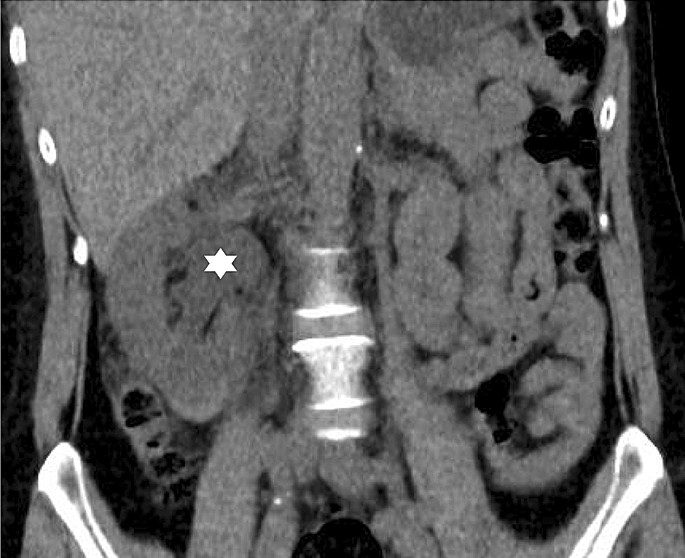
7/ Pain lasting more than 12 hours - 4 %;
due to ureteral obstruction from a blood clot or
stretching of the renal capsule by a subcapsular hematoma
Image: Ureteric obstruction due to blood clot
link.springer.com/article/10.100…
due to ureteral obstruction from a blood clot or
stretching of the renal capsule by a subcapsular hematoma
Image: Ureteric obstruction due to blood clot
link.springer.com/article/10.100…
8/AVF - 14 %
due to damage to the walls of an adjacent artery and vein usually clinically silent and resolve spontaneously over 1 to 2 years.
👁🗨Diagnosis - color Doppler ultrasonography or arteriography
👁🗨Treatment - transcatheter arterial embolization or surgical ligation
due to damage to the walls of an adjacent artery and vein usually clinically silent and resolve spontaneously over 1 to 2 years.
👁🗨Diagnosis - color Doppler ultrasonography or arteriography
👁🗨Treatment - transcatheter arterial embolization or surgical ligation

9/ Chronic hypertension due to the "Page kidney"
Pressure-induced ischemia from a large subcapsular hematoma → activation of RAS→ HTN
radiopaedia.org/articles/page-…
pubmed.ncbi.nlm.nih.gov/1951341/
Pressure-induced ischemia from a large subcapsular hematoma → activation of RAS→ HTN
radiopaedia.org/articles/page-…
pubmed.ncbi.nlm.nih.gov/1951341/
10/Perirenal soft tissue infection - 0.2 %,🦠
most often in patients with active parenchymal renal infection
pubmed.ncbi.nlm.nih.gov/1395165/
most often in patients with active parenchymal renal infection
pubmed.ncbi.nlm.nih.gov/1395165/
11/Rarely, puncture of the
📌liver,
📌pancreas,
📌spleen, or
📌even aorta may occur, as well as
📌urinoma formation from puncture of the urinary tract
pubmed.ncbi.nlm.nih.gov/25115496/
📌liver,
📌pancreas,
📌spleen, or
📌even aorta may occur, as well as
📌urinoma formation from puncture of the urinary tract
pubmed.ncbi.nlm.nih.gov/25115496/
12/ The risk of bleeding associated with transjugular kidney biopsies is unclear, and which patients are the best candidates for this route is unknown.
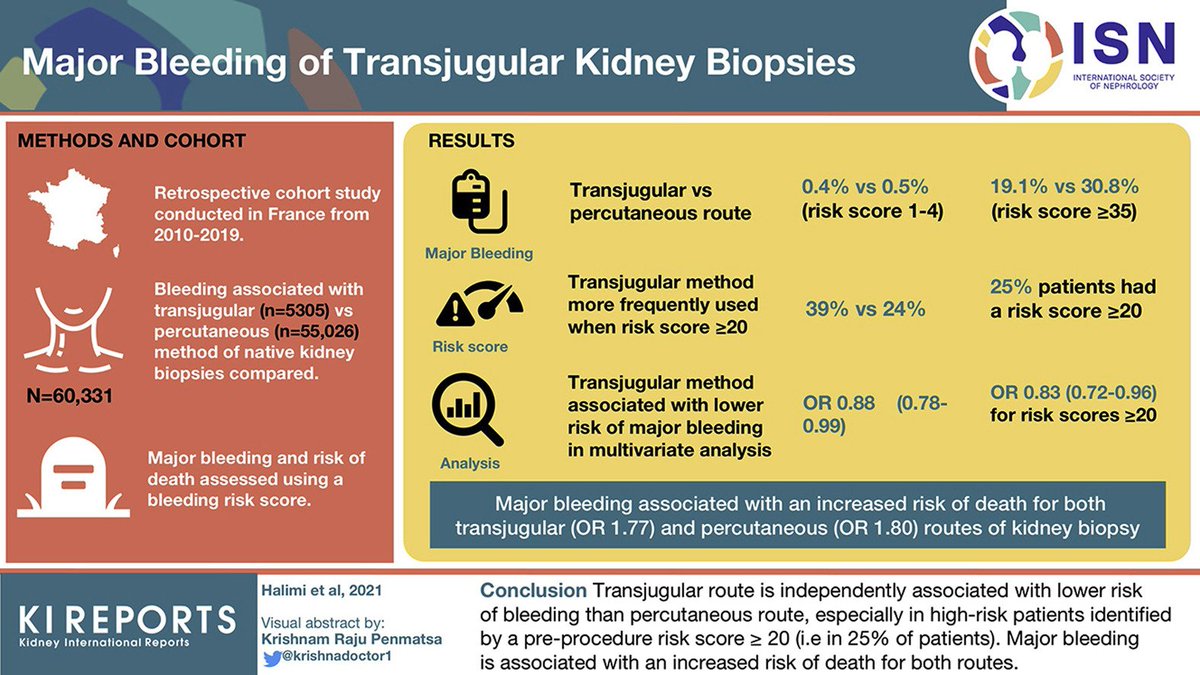
13/ Methods:
📌France (2010–2019)🇫🇷
📌Retrospective cohort study 🧑🤝🧑
📌bleeding associated with transjugular vs percutaneous native kidney biopsies 🩸
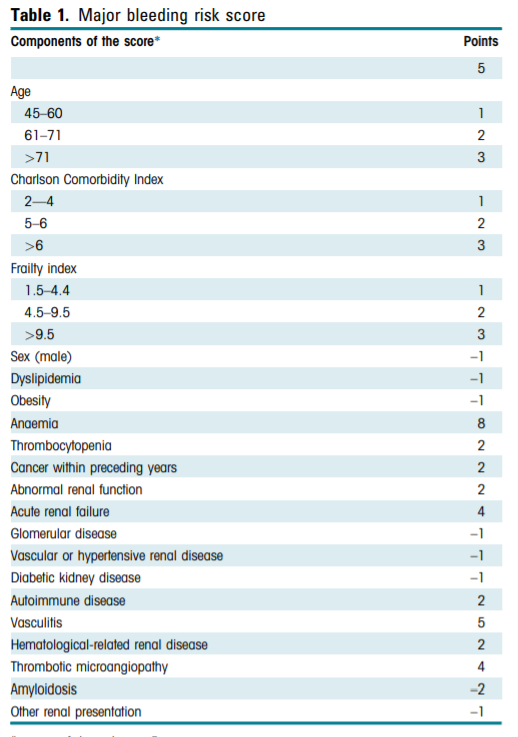
📌Outcomes: Major bleeding 🩸at day 8 and risk of death ☠️at day 30 assessed using Bleeding risk score
📌France (2010–2019)🇫🇷
📌Retrospective cohort study 🧑🤝🧑
📌bleeding associated with transjugular vs percutaneous native kidney biopsies 🩸
📌Outcomes: Major bleeding 🩸at day 8 and risk of death ☠️at day 30 assessed using Bleeding risk score
14/ Results:
#⃣Total 60,331 patients (transjugular route: 5305; percutaneous route: 55,026 patients)
🩸Transjugular ↓ risk of major bleeding than percutaneous [OR]: 0.88 [0.78–0.99]), especially for scores ≥20
#⃣Total 60,331 patients (transjugular route: 5305; percutaneous route: 55,026 patients)
🩸Transjugular ↓ risk of major bleeding than percutaneous [OR]: 0.88 [0.78–0.99]), especially for scores ≥20
15/ Major bleeding 🩸was associated with an ⬆️ risk of death☠️ both for transjugular (OR: 1.77 [1.00–3.14]) and percutaneous (OR: 1.80 [1.43–2.28]) routes.
kireports.org/article/S2468-…
kireports.org/article/S2468-…
16/Conclusion: transjugular route : ⬇️ risk of bleeding 🩸than percutaneous route, especially in high-risk patients with pre-procedure risk score ≥20 (i.e., 25% of patients). Major bleeding is associated with an ⬆️risk of death for both routes.
This tweetorial is brought to you by @nephromythri on behalf of @KIReports social media team
• • •
Missing some Tweet in this thread? You can try to
force a refresh



