Acute pancreatitis is very common, yet there are no approved therapies 



Acute pancreatitis is on the rise.

Death from idiopathic pancreatitis is decreasing


Once you've confirmed AP, get imaging, calcium, TGs, and look at meds

Note: just because RUQ US is normal doesn't mean biliary is the cause. Microlithiasis is not well visualized.

Cholecystectomy ⬇️ the risk of recurrent idiopathic AP.
1 in 5 chance!
1 in 5 chance!

For obstruction, repeat imaging in a few months.
Don't forget ductal disruptions!
Don't forget ductal disruptions!



If TGs >1000, can be the cause.

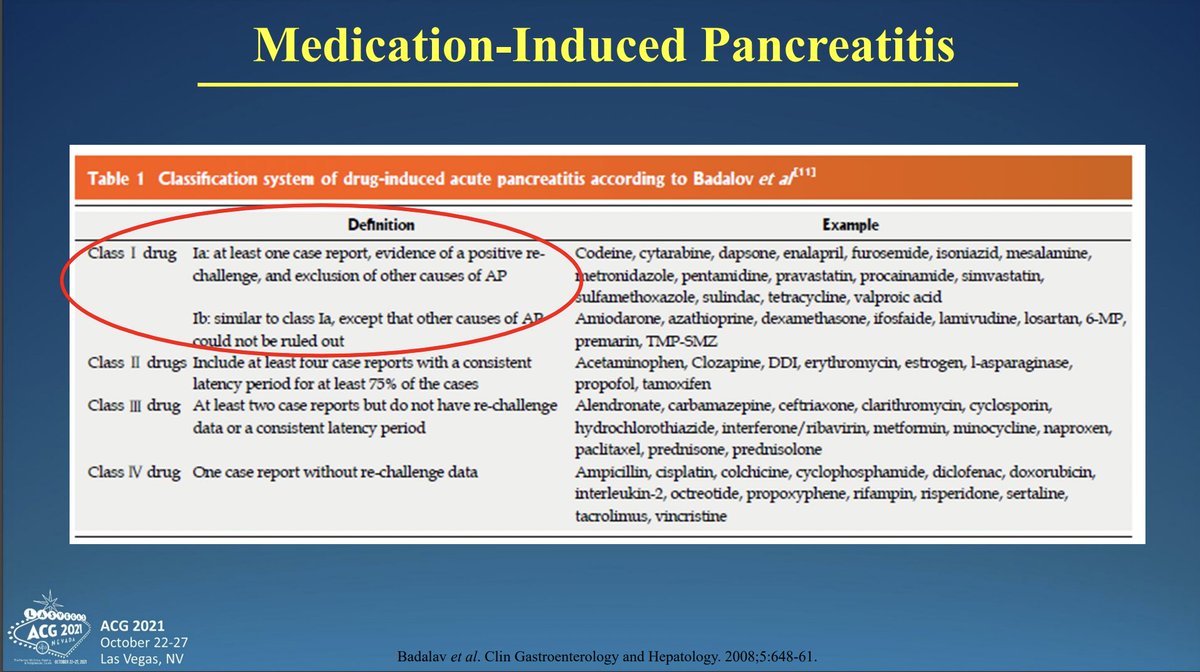
Excellent reference for medication-induced AP
We continue to refine our understanding of genetic causes of AP.
Think in young patients with recurrent AP.
Think in young patients with recurrent AP.

Type I autoimmune: IgG4 related
Type II autoimmune pancreatitis: younger patients, associated with #IBD, can only diagnose with pancreatic biopsy
Type II autoimmune pancreatitis: younger patients, associated with #IBD, can only diagnose with pancreatic biopsy

Why fluid resuscitation in AP? Poor arterial supply makes the pancreas exquisitely sensitive to hypovolemia, which worsens the disease process.
‼️LR is superior to NS!!!
Get BUN in 8hrs, modify if needed, watch for abdominal compartment syndrome
‼️LR is superior to NS!!!
Get BUN in 8hrs, modify if needed, watch for abdominal compartment syndrome



NO mortality benefit for antibiotics in AP.
With infected pancreatic necrosis, treat medically with antibiotics. "Keep the surgeons away from them!"
With infected pancreatic necrosis, treat medically with antibiotics. "Keep the surgeons away from them!"



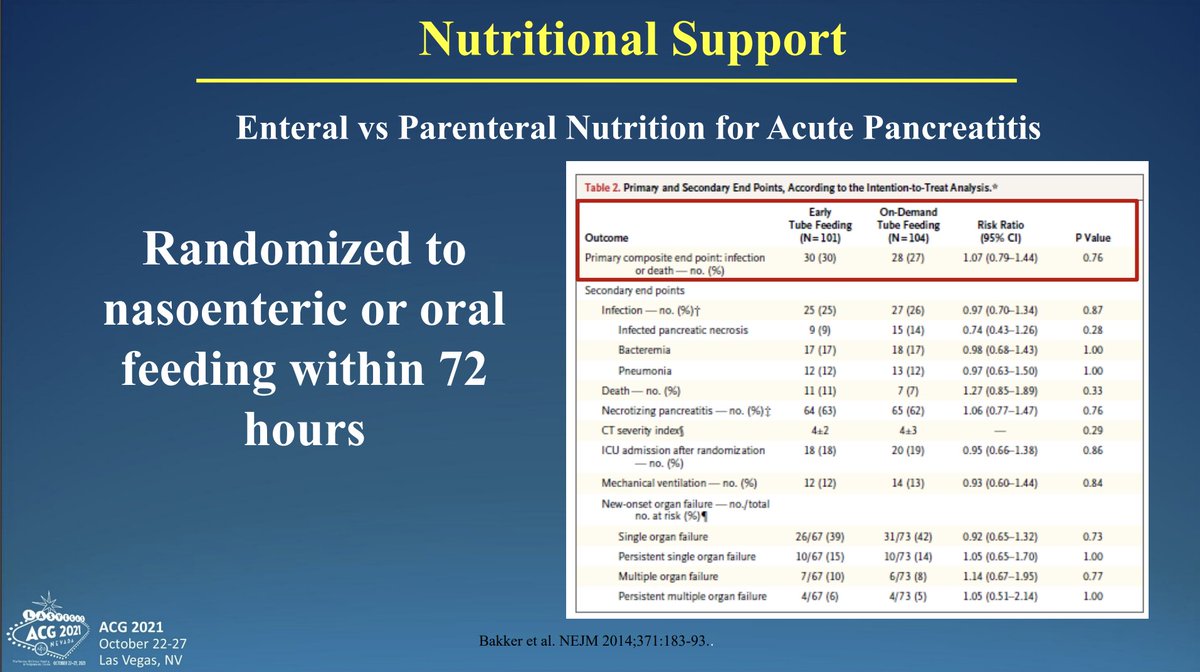
USE THE GUT: "Resting the pancreas? That's 1970s medicine."
NG tube only if aspiration risk.
NG tube only if aspiration risk.






Hope for the future: many clinical trials out there for acute pancreatitis! More research needed!

• • •
Missing some Tweet in this thread? You can try to
force a refresh