🥊 #HitMeWithYourBestShot: Reguiero vs Siegel
@MRegueiroMD➕anti-TNFs "Why wouldn't we use anti-TNF as first line #IBD therapy?!"
#AIBD2021 @IBDConference @DrCoreySiegel
@MRegueiroMD➕anti-TNFs "Why wouldn't we use anti-TNF as first line #IBD therapy?!"
#AIBD2021 @IBDConference @DrCoreySiegel




Anti-TNFs are EFFECTIVE




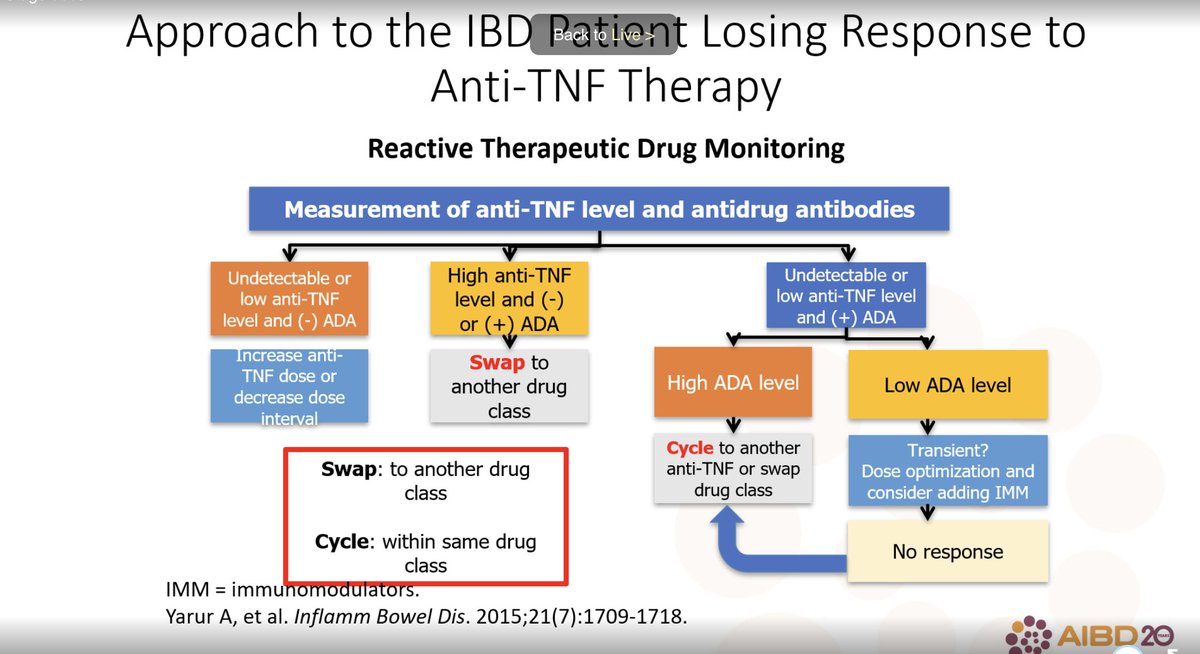
We know a LOT about #TDM in anti-TNFs

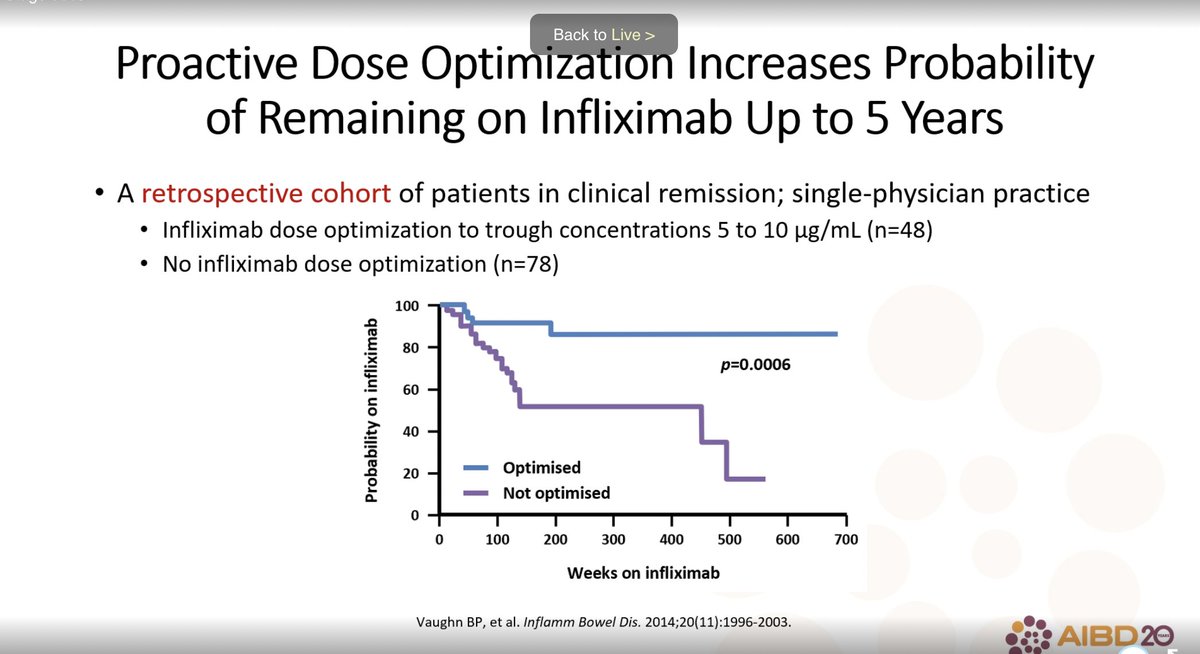

We have PRECISION MEDICINE with anti-TNFs

Anti-TNFs
⬆️infections, but otherwise very safe
⬆️infections, but otherwise very safe

Anti-TNFs work for MULTIPLE ASPECTS of #IBD, especially fistulae

Anti-TNFs are effective for POSTOP CROHN DISEASE


Anti-TNFs are THE BEST treatment for EIMs

ACESS is easiest with anti-TNFs
Think of biosimilars like fingerprints
Think of biosimilars like fingerprints




"Dr. @DrCoreySiegel, @DartmouthHitch gastroenterologist, scientist, and future Nobel Prize winner 🏅: -@MRegueiroMD 😂

Cons of non anti-TNF biologics


@MRegueiroMD: start with anti-TNFs

@DrCoreySiegel: anything BUT anti-TNF!
Many factors go into choosing the right therapy for the right patient
Many factors go into choosing the right therapy for the right patient

The data for safety of VDZ and UST speak for themselves. "Probably as safe as not being on any drug in terms of side effects."


While there is a small ⬆️ risk of lymphoma and skin cancers in anti-TNFs, there is NO risk of cancers in vedolizumab or ustekinumab.

"@MRegueiroMD, this is YOUR safety pyramid!" 😂
While efficacy is about equivalent, safety is better for VDZ/UST
While efficacy is about equivalent, safety is better for VDZ/UST

Need to consider the efficacy and safety profile of COMBO therapy with anti-TNFs

Immunogenicity is highest for anti-TNFs

From real world EVOLVE-UC, it doesn't matter if we start or end at anti-TNF. So we CAN try non-TNFs first without worry.

Ustekinumab used first ⬆️⬆️⬆️⬆️QALYs

How to select first biologic:
Apart from ASUC and perianal CD, the efficacy of TNFs and non-TNFs are basically the same. The non-TNFs are safer. We don't lose efficacy of TNF if we start with non-TNF.
Shared decision making with patient! 🤝
Apart from ASUC and perianal CD, the efficacy of TNFs and non-TNFs are basically the same. The non-TNFs are safer. We don't lose efficacy of TNF if we start with non-TNF.
Shared decision making with patient! 🤝

@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh