
1/ Shortish thread about FGF21, a hormone secreted by the liver, muscles and other tissues that is profoundly interesting.
👉 Regulates lipids (HDL, LDL, LPL, ApoCIII and more)
👉 FGF21 analogs are being explored as a treatment for obesity, type II diabetes, NAFLD
👉 Regulates lipids (HDL, LDL, LPL, ApoCIII and more)
👉 FGF21 analogs are being explored as a treatment for obesity, type II diabetes, NAFLD

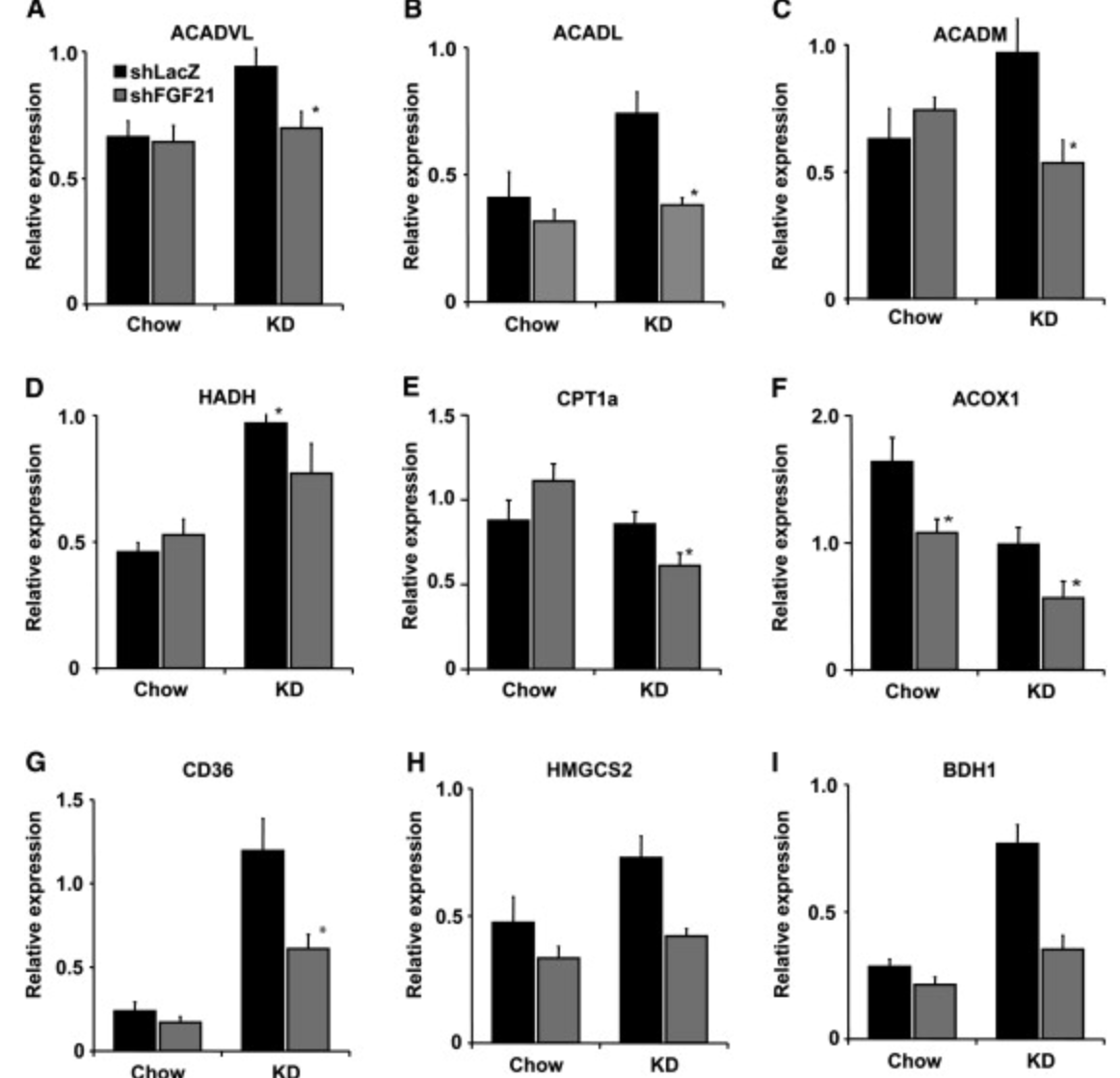
2/ FGF21 really caught my attention when I read this paper, which provides compelling evidence that FGF21 is essential for in ketosis and lipid oxidation in mice on a ketogenic diet.
cell.com/cell-metabolis…
cell.com/cell-metabolis…
3/ Ketogenic diet increased GF21 levels ~20-fold and knockdown of FGF21 created severe metabolic impairments including decreased ketones, hypertriglyceridemia, fatty liver, and decreased expression of ton of genes involved in lipid and ketone metabolism
4/ The axis of activity seems to be:
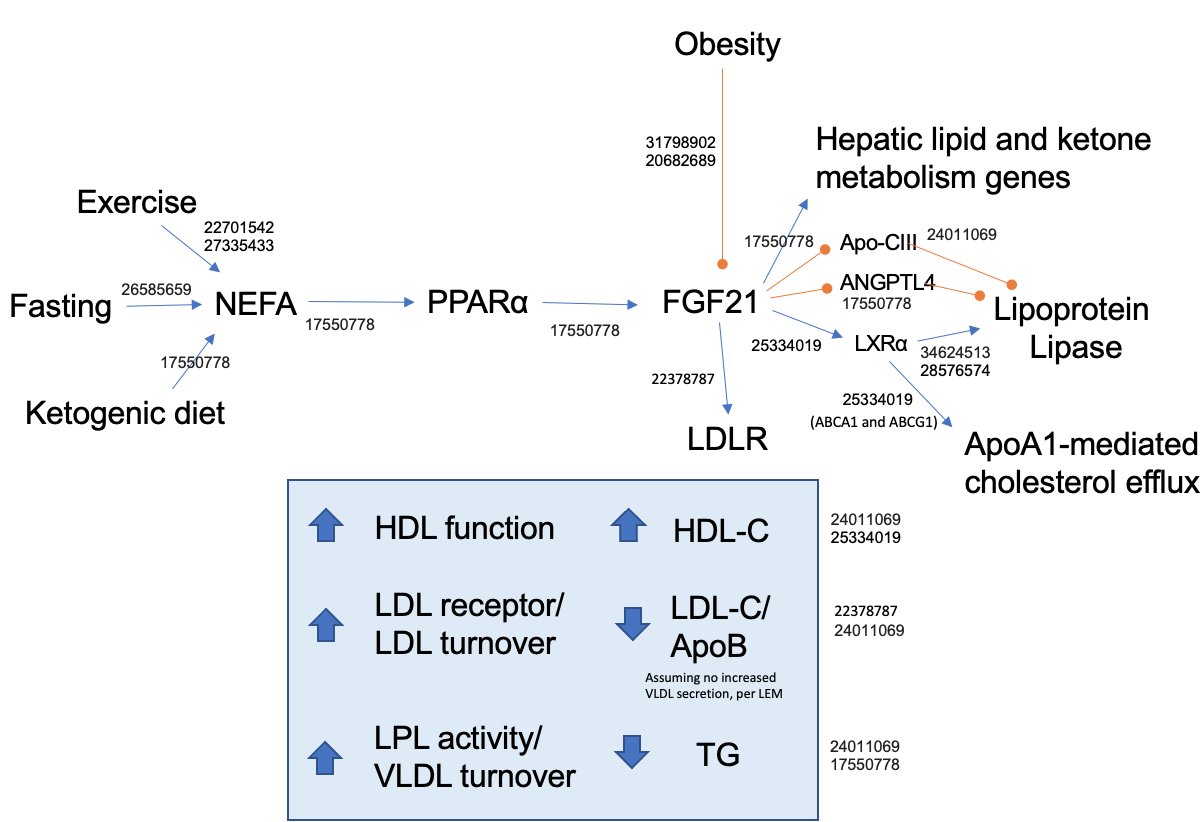
Increased lipolysis➡️ NEFA➡️activation of PPARalpha transcription factor➡️ induction of FGF21 ➡️ regulation of genes involved in ketosis and lipid metabolism
In effect, FGF21 may be one of the key signals regulating fat adaptation
Increased lipolysis➡️ NEFA➡️activation of PPARalpha transcription factor➡️ induction of FGF21 ➡️ regulation of genes involved in ketosis and lipid metabolism
In effect, FGF21 may be one of the key signals regulating fat adaptation
5/ There is now energized debate over wether #obesity represents "FGF21 resistant state", analogous to insulin resistance (and FGF21 levels are associated w/ BMI, TG, and HOMA-IR/Matsuda index)
I wonder what @BenBikmanPhD thinks?
pubmed.ncbi.nlm.nih.gov/31798902/
pubmed.ncbi.nlm.nih.gov/20682689/
I wonder what @BenBikmanPhD thinks?
pubmed.ncbi.nlm.nih.gov/31798902/
pubmed.ncbi.nlm.nih.gov/20682689/
6/ There is also interest in exploring FGF21 analogs and pathway activators as a treatment for type 2 diabetes, obesity, and NAFLD
nature.com/articles/s4157…
nature.com/articles/s4157…
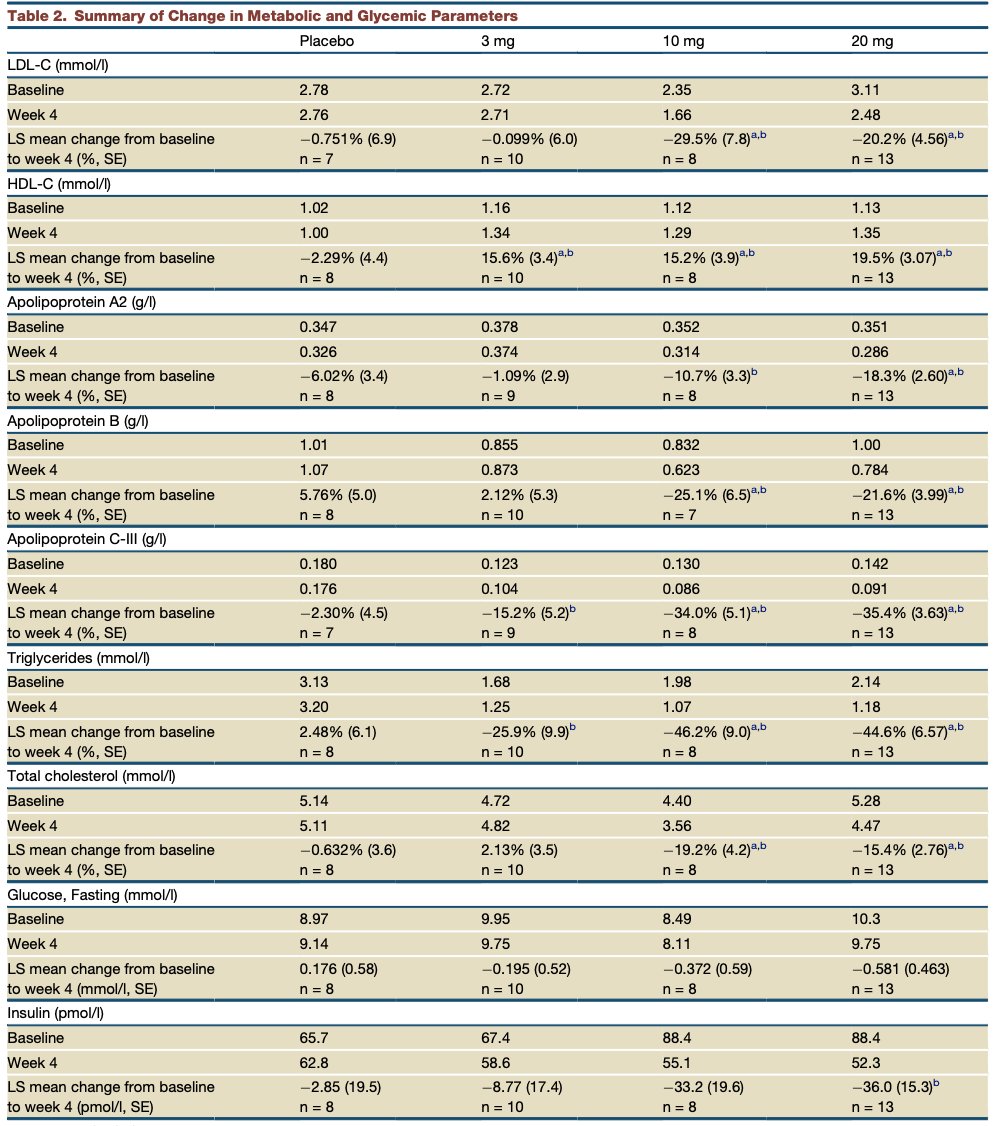
7/ Some of the results look quite impressive, with changes in LDL/ApoB, HDL, ApoCIII, TG and more
pubmed.ncbi.nlm.nih.gov/24011069/
(These data are from Lilly's LY2405319 trial. I'm curious what @ethanjweiss @Lpa_Doc might know about this trial?)
pubmed.ncbi.nlm.nih.gov/24011069/
(These data are from Lilly's LY2405319 trial. I'm curious what @ethanjweiss @Lpa_Doc might know about this trial?)
8/ I'm definitely largely ignorant about FGF21, but I find it very interesting and wanted to share. Thoughts from all those not mentioned already welcome @realDaveFeldman @Ad_SotoMota @lowcarbGP @hubermanlab @drbenbo @ everyone.
Oh, and good morning!
Oh, and good morning!
9/ Summary slide
• • •
Missing some Tweet in this thread? You can try to
force a refresh





