JUST IN [Thread] 1. Early findings from 2 SA studies suggest #Omicron has a much higher rate of asymptomatic "carriage" (#COVID19 without symptoms) than previous variants and this is likely an important reason why the variant spreads so fast.
Preprint: bit.ly/3q8NykS
Preprint: bit.ly/3q8NykS


2. Which studies are findings based on?
1. Ubuntu: A sub-Saharan #Africa study that measures the effectiveness of #Moderna's #COVID19 jab in #HIV+ people (all initial sites in SA)
2. A sub-study of #Sisonke, conducted among SA #HealthWorkers, that measures #JnJ's effectiveness
1. Ubuntu: A sub-Saharan #Africa study that measures the effectiveness of #Moderna's #COVID19 jab in #HIV+ people (all initial sites in SA)
2. A sub-study of #Sisonke, conducted among SA #HealthWorkers, that measures #JnJ's effectiveness
3. Neither of the studies = designed 2 look @ asymptomatic infections specifically, rather 2 measure breakthrough infections, immunogenicity + effectiveness of jabs in HIV+ and other groups, but they do give useful info on how #Omicron's spread differs from other variants.
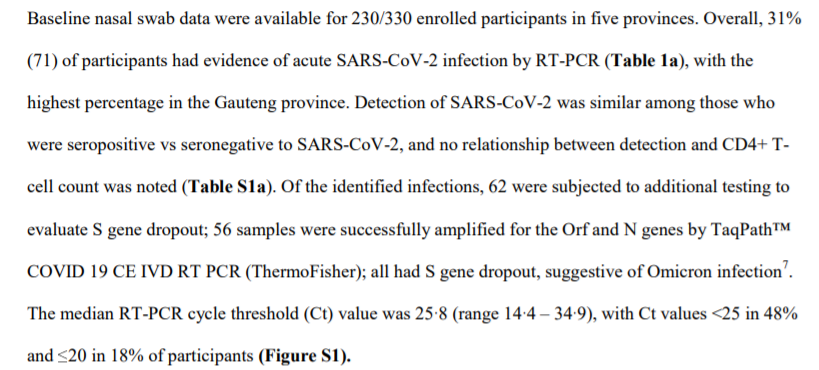
4. What did the Ubuntu study show?
- Study period: 2 - 17 Dec
- 31% of unvaccinated volunteers had #COVID19 without symptoms (71/230 participants)
- This is in sharp contrast with pre-#Omicron studies: During ancestral, Beta + Delta variants rates = 1%-2.6%, so 7-12x lower
- Study period: 2 - 17 Dec
- 31% of unvaccinated volunteers had #COVID19 without symptoms (71/230 participants)
- This is in sharp contrast with pre-#Omicron studies: During ancestral, Beta + Delta variants rates = 1%-2.6%, so 7-12x lower

5. What did #Sisonke find?
- Study period: mid-November to Dec 7
- 2.6% of vaccinated (with #JnJ) volunteers had #COVID19 without symptoms during the Beta and Delta outbreaks. With #Omicron this rose to 16% (91/577 participants)
- Study period: mid-November to Dec 7
- 2.6% of vaccinated (with #JnJ) volunteers had #COVID19 without symptoms during the Beta and Delta outbreaks. With #Omicron this rose to 16% (91/577 participants)

6. How did researchers know asymptomatic carriers were infected with #Omicron?
1. Proportions of the samples were sequenced
2. They looked at PCR test results (if a certain gene, called an S gene, was not picked up, it indicated it was Omicron (this is known as S gene dropout)
1. Proportions of the samples were sequenced
2. They looked at PCR test results (if a certain gene, called an S gene, was not picked up, it indicated it was Omicron (this is known as S gene dropout)
7. What do the (early) findings mean?
1. #Omicron infection possibly results in a higher % of people with asymptomatic #COVID19 than other variants
2. This likely plays an NB role in its fast spread — even among populations with high prior rates of #SARSCOV2 infection (like SA)
1. #Omicron infection possibly results in a higher % of people with asymptomatic #COVID19 than other variants
2. This likely plays an NB role in its fast spread — even among populations with high prior rates of #SARSCOV2 infection (like SA)

8. Many of the asymptomatic carriers in the studies had high nasal viral titers (so a lot of virus) — suggesting that sub-clinical carriage (so disease without symptoms) could be a major reason why #Omicron is spreading so fast globally.
Press release: bit.ly/3GlD1bS
Press release: bit.ly/3GlD1bS
9. What does this study not tell us?
How #COVID19 vaccination affects asymptomatic infection and such people's ability to infect other people
Why not?
1. All Ubuntu samples = unvaccinated people
2. #Sisonke sub-study's sample size = 2 small 2 calculate vaccine effectiveness
How #COVID19 vaccination affects asymptomatic infection and such people's ability to infect other people
Why not?
1. All Ubuntu samples = unvaccinated people
2. #Sisonke sub-study's sample size = 2 small 2 calculate vaccine effectiveness

• • •
Missing some Tweet in this thread? You can try to
force a refresh