
1) Welcome to our new #tweetorial on optimizing #interprofessional & #multidisciplinary care & medical therapy for patients with #DKD. I am Sophia Ambruso DO, @Sophia_kidney, from @CU_kidney. 

2) This #accredited #tweetorial series on #kidneydisease #DKD through the lens of #T2D is supported by an independent educational grant from the Boehringer Ingelheim/Lilly Alliance and is intended for healthcare providers. Faculty disclosures are at ckd-ce.com/disclosures/.
3) This activity is accredited for 0.75h credit for #physicians #physicianassociates #nurses #NPs #pharmacists. Past programs still eligible for credit can be found at ckd-ce.com. FOLLOW US for more programs by expert faculty!
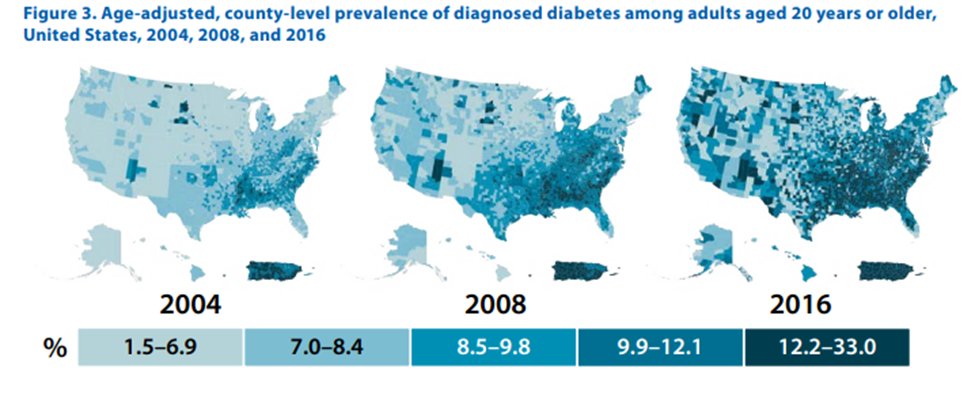
4) We must view the optimal approach to #DKD in the context of #DM as a global health crisis, affecting
~27-31 million ppl (8.2% of US population)
~400 million ppl worldwide
🔓cdc.gov/diabetes/pdfs/…
~27-31 million ppl (8.2% of US population)
~400 million ppl worldwide
🔓cdc.gov/diabetes/pdfs/…
5) As of 2018, crude prevalence of #ESKD attributable to diabetes was 38.6%. Diabetes is the leading cause of #CKD worldwide, accounting for up to 50% of all patients with ESKD.
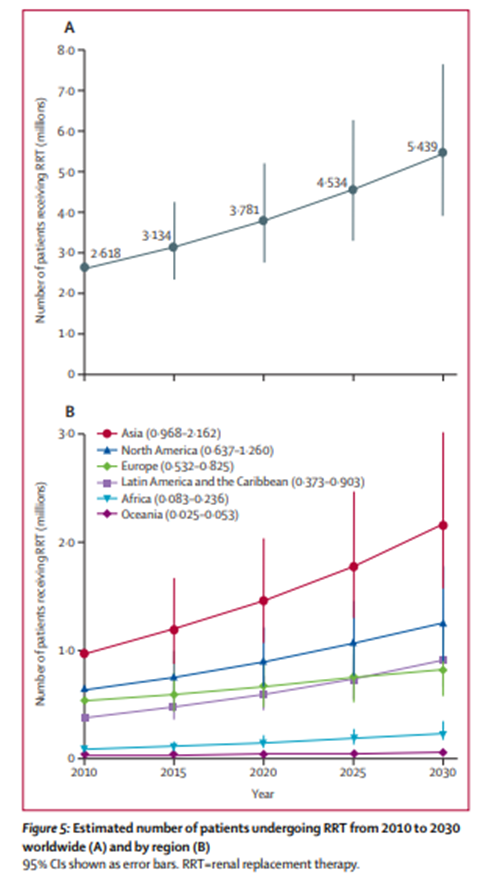
6) Based on a study in 2015, the world use of kidney replacement therapy #KRT is projected to double by 2030, highlighting the #CKD disease burden and global challenges ahead.
doi.org/10.1016/s0140-…
doi.org/10.1016/s0140-…
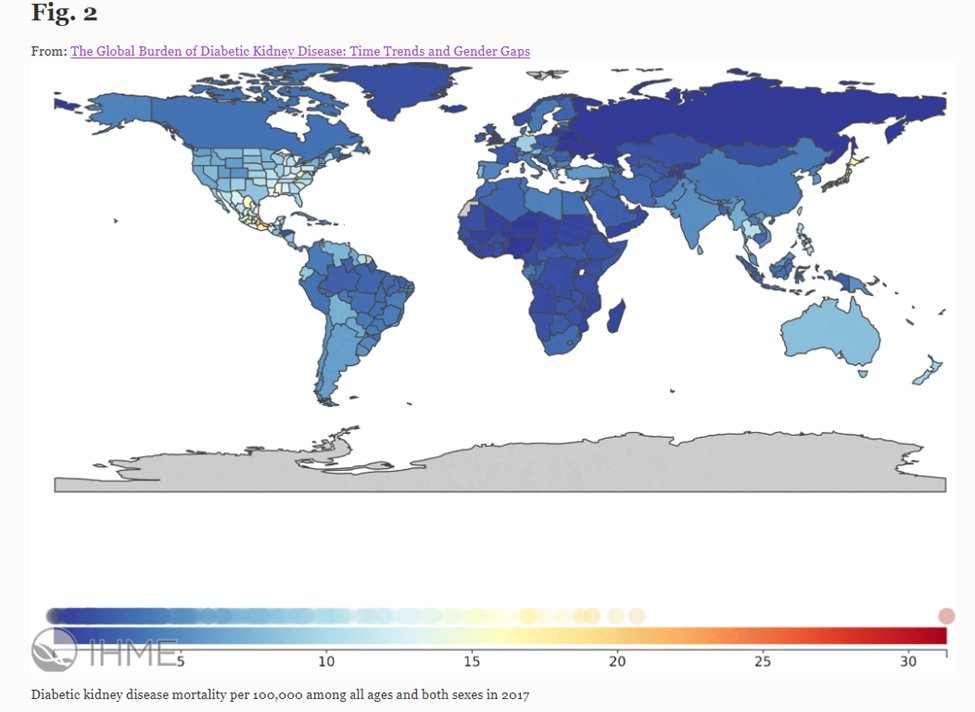
7) There were an estimated 219,451 deaths attributed to diabetic kidney disease #DKD, ➡️approximately 35% of ALL CKD deaths in 2017 worldwide.
See below: diabetic kidney disease mortality per 100,000 worldwide in 2017
🔓link.springer.com/article/10.100…
See below: diabetic kidney disease mortality per 100,000 worldwide in 2017
🔓link.springer.com/article/10.100…
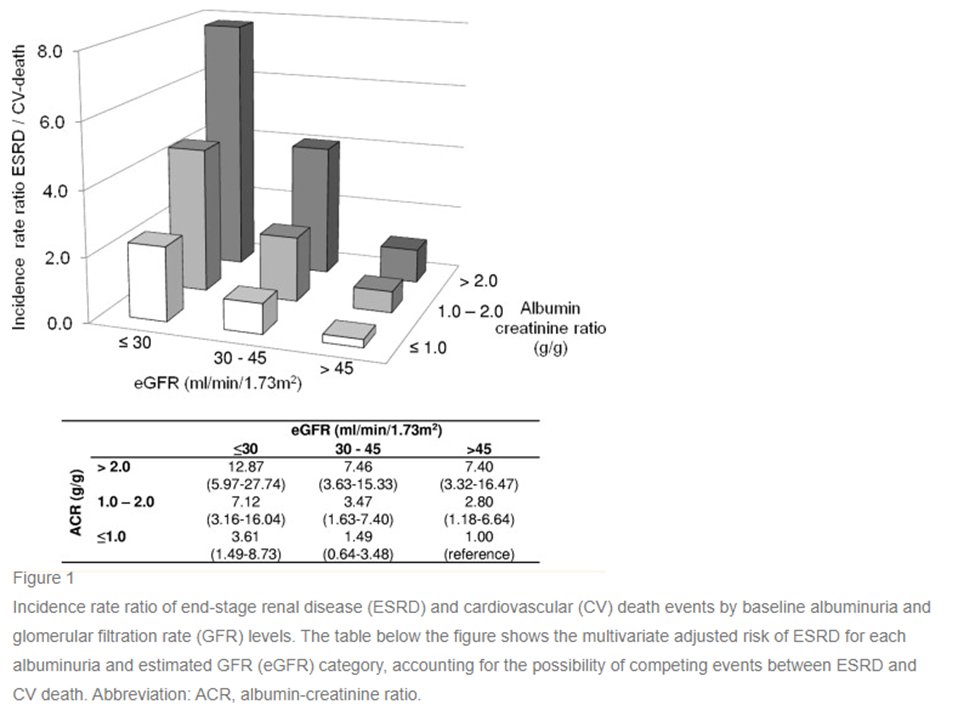
8) The combination #DM+#CKD ➡️independent & additive effect on #CV risk & mortality.
For every halving of #eGFR, CV incidence is 2x higher.
For every 10x ⬆️in baseline urine albumin, CV event incidence is 2.5x higher.
🔓pubmed.ncbi.nlm.nih.gov/22051245/
🔓ncbi.nlm.nih.gov/pmc/articles/P…
For every halving of #eGFR, CV incidence is 2x higher.
For every 10x ⬆️in baseline urine albumin, CV event incidence is 2.5x higher.
🔓pubmed.ncbi.nlm.nih.gov/22051245/
🔓ncbi.nlm.nih.gov/pmc/articles/P…

9) #CKD itself contributes to disease burden with dramatic impacts on quality of life in advanced #CKD and #dialysisdependent #ESKD made worse by #T2D
doi.org/10.2215/CJN.08…
ncbi.nlm.nih.gov/pmc/articles/P…
doi.org/10.2215/CJN.08…
ncbi.nlm.nih.gov/pmc/articles/P…
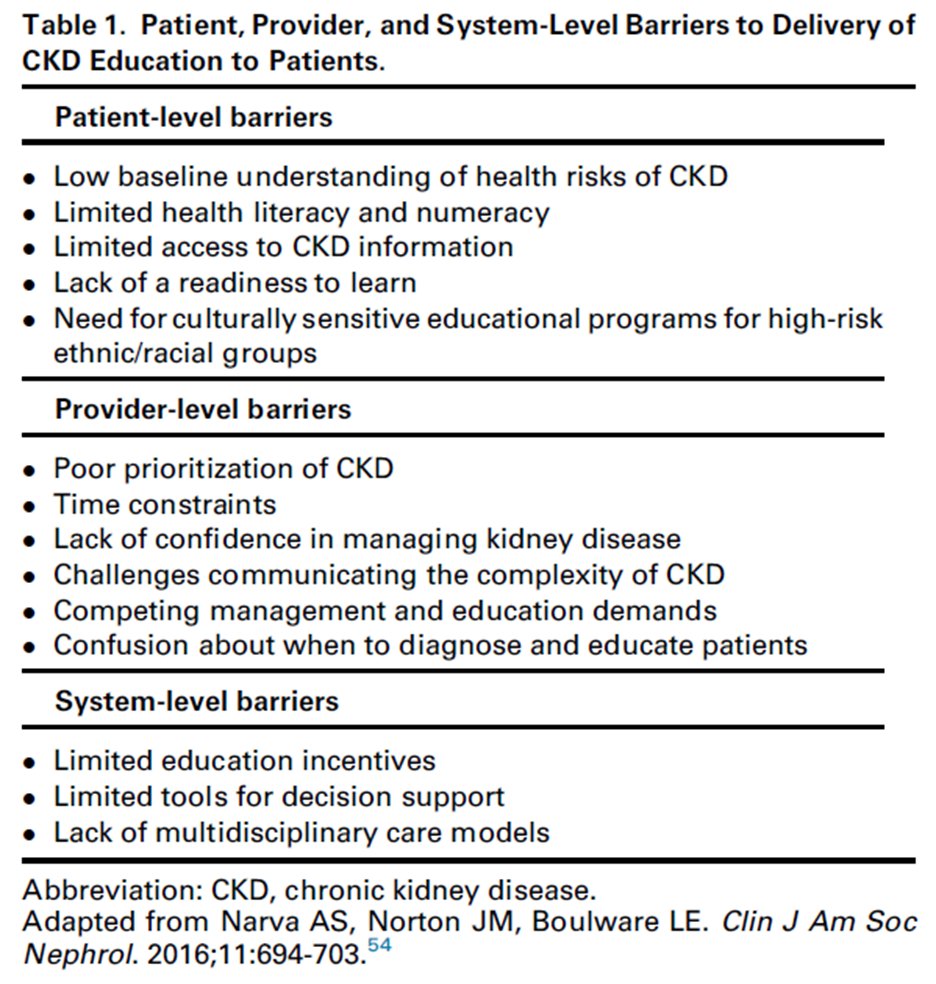
10) To get ahead of & reduce the impact #T2D & #DKD, coordinated efforts for early ID & intervention are necessary to slow disease progression. While the medical community has made strides, gaps & barriers at patient, physician, & system levels remain
doi.org/10.1053/j.ackd…
doi.org/10.1053/j.ackd…
11) One in 7 of US adults have CKD, 90% of whom don’t know it. Moreover, 40% with SEVERE CKD don’t know they have CKD
🔓cdc.gov/kidneydisease/…
🔓cdc.gov/kidneydisease/…
12) An estimated 90% of patients with #DKD are undiagnosed & 40% with severe #DKD go undiagnosed
doi.org/10.1053/j.ackd…
doi.org/10.1053/j.ackd…
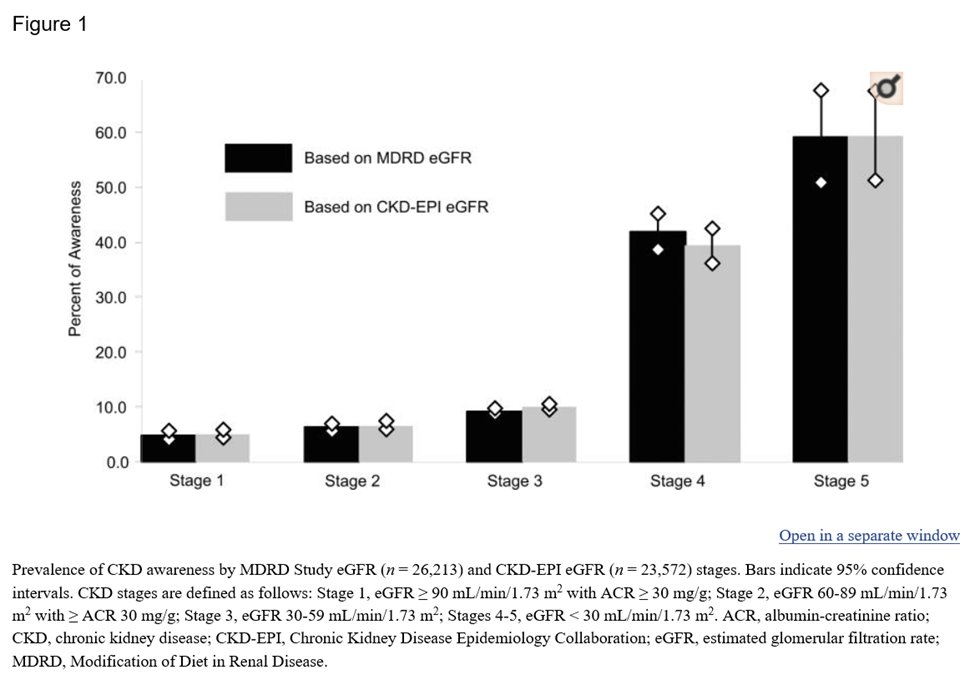
13) With disease progression comes increased #CKD awareness, 40% with CKD IV and 60% with CKD V.
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
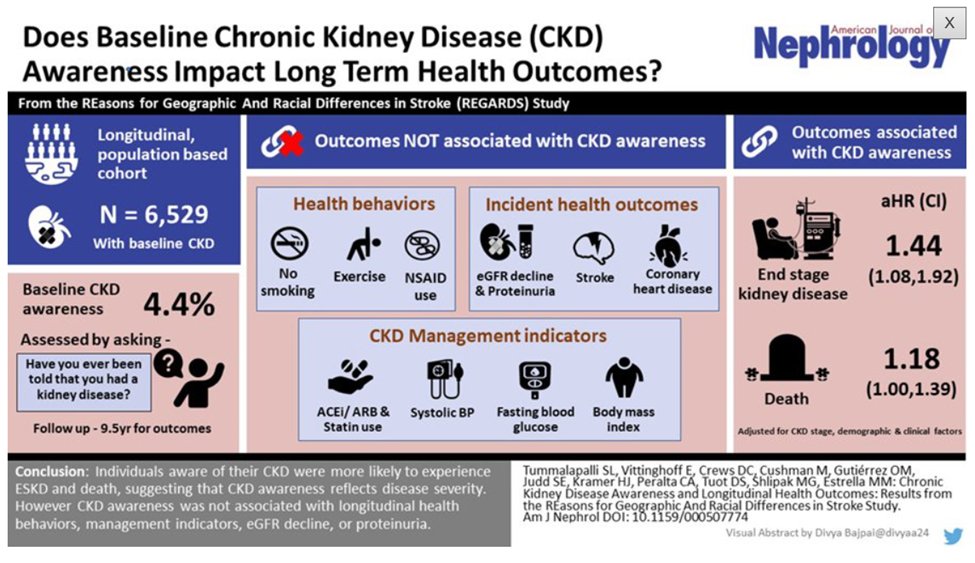
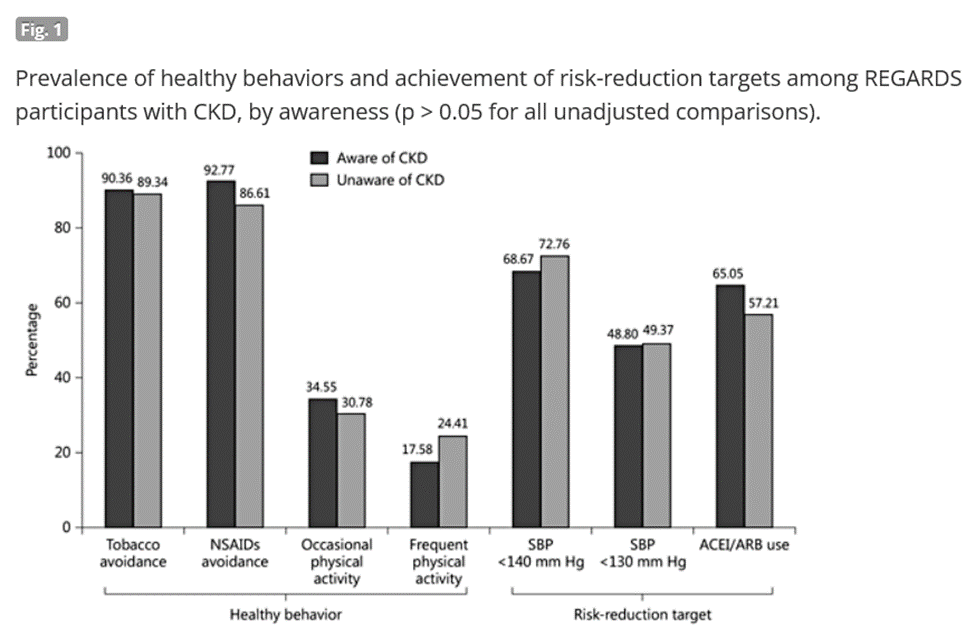
14) However, CKD awareness does not by itself lead to healthy, risk reduction behaviors ie. tobacco/NSAID avoidance, exercise, ACEi/ARB use; suggesting barriers at the patient & provider level
ncbi.nlm.nih.gov/pmc/articles/P…
karger.com/Article/FullTe…
ncbi.nlm.nih.gov/pmc/articles/P…
karger.com/Article/FullTe…
15) The recognition of #CKD by medical professionals has increased from 2006-2009 to 2014-2017, where coding for CKD increased from 3.252.3%. However, still almost half of patients with CKD go undiagnosed.
jamanetwork.com/journals/jaman…
jamanetwork.com/journals/jaman…
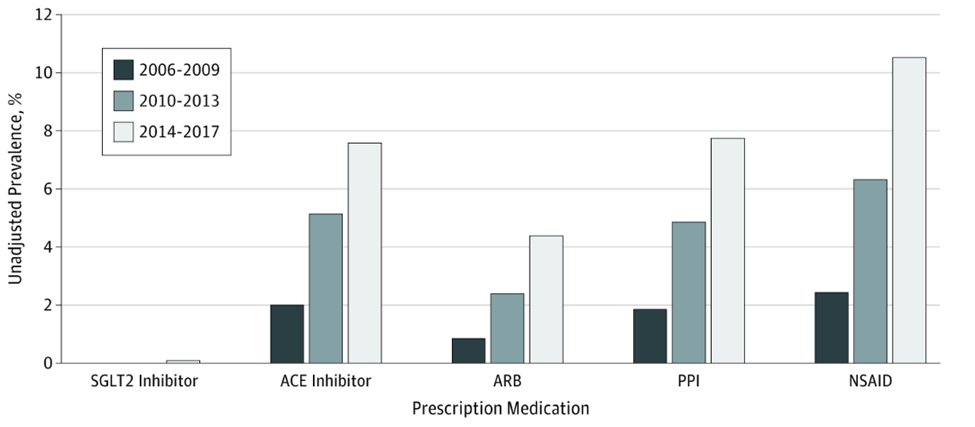
16) Physicians still underprescribe proven #renoprotective meds, and overprescribe potentially harmful drugs. Below is unadjusted prevalence of prescription drugs #SGLT2i, #ACEi, #ARB, #PPI, #NSAID in CKD 3a-5
🔓 jamanetwork.com/journals/jaman…
🔓 jamanetwork.com/journals/jaman…
17) In short, barriers persist in #DKD awareness, detection and provision of evidence-based interventions at the patient, provider and systemic levels.
18) Fortunately, there are existing and emerging, evidence-based therapies that provide new hope in management of #T2D and #DKD and possibilities an improved #DKD global trajectory
19) So, to kick off our discussion of treatment, tell me, the most familiar renoprotective agents in #DKD known to alter glomerular hemodynamics are which of these?
20) Mark your best answer and return tomorrow for a continuation of this program—we will focus on TEAM management! @NWiegley @kkalra_22 @ghobby @priti899 @JohnRMontford @NamrataYParikh @CharlieTomson @DiMiRenalMD @KIDNEYcon @GlomCon @MedTweetorials #FOAMed @aakashshingada
21) Welcome back! We are focusing on optimizing #interprofessional & #multidisciplinary #TEAMWORK in the management of #diabetic #kidneydisease #DKD. I am @sophia_kidney and YOU are earning 🆓CE/#CME! 👏to @divyaa24 @rheault_m @ChristosArgyrop @nephondemand @edgarvlermamd
22) The goal of #DKD treatment is three-fold:
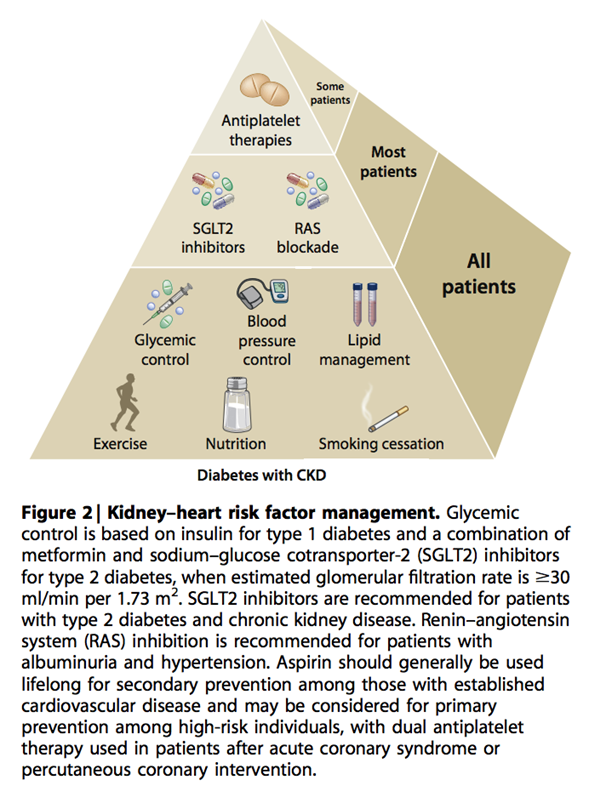
I. reduce concurrent or continued injury by addressing modifiable risk factors
--Glycemic control (goal A1c <7)
--Weight loss
--Smoking cessation
--BP control (goal <130/80)
--Low salt diet
🔓ajkd.org/article/S0272-…
I. reduce concurrent or continued injury by addressing modifiable risk factors
--Glycemic control (goal A1c <7)
--Weight loss
--Smoking cessation
--BP control (goal <130/80)
--Low salt diet
🔓ajkd.org/article/S0272-…
23) Goal of #DKD treatment is three-fold:
II. medicines that improve glomerular hemodynamics
III. medicines with anti-inflammatory/antifibrotic activity
🔓ajkd.org/article/S0272-…
II. medicines that improve glomerular hemodynamics
III. medicines with anti-inflammatory/antifibrotic activity
🔓ajkd.org/article/S0272-…
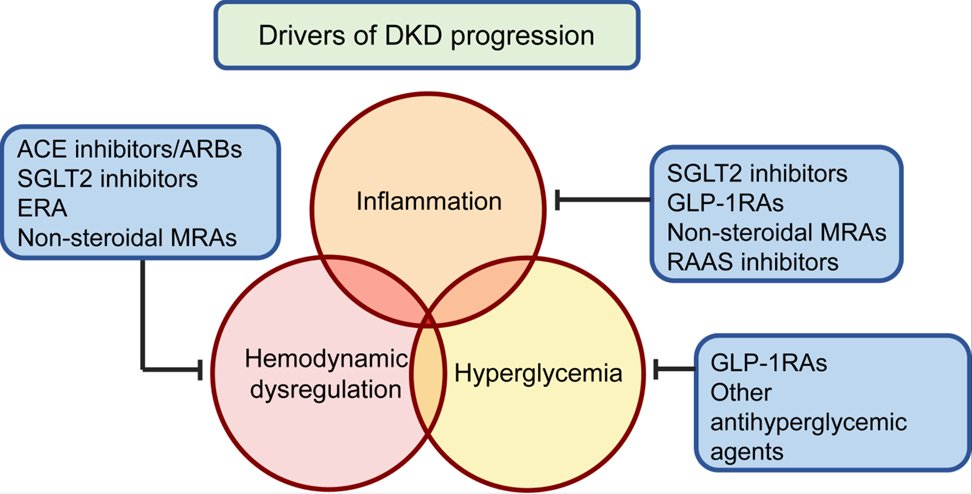
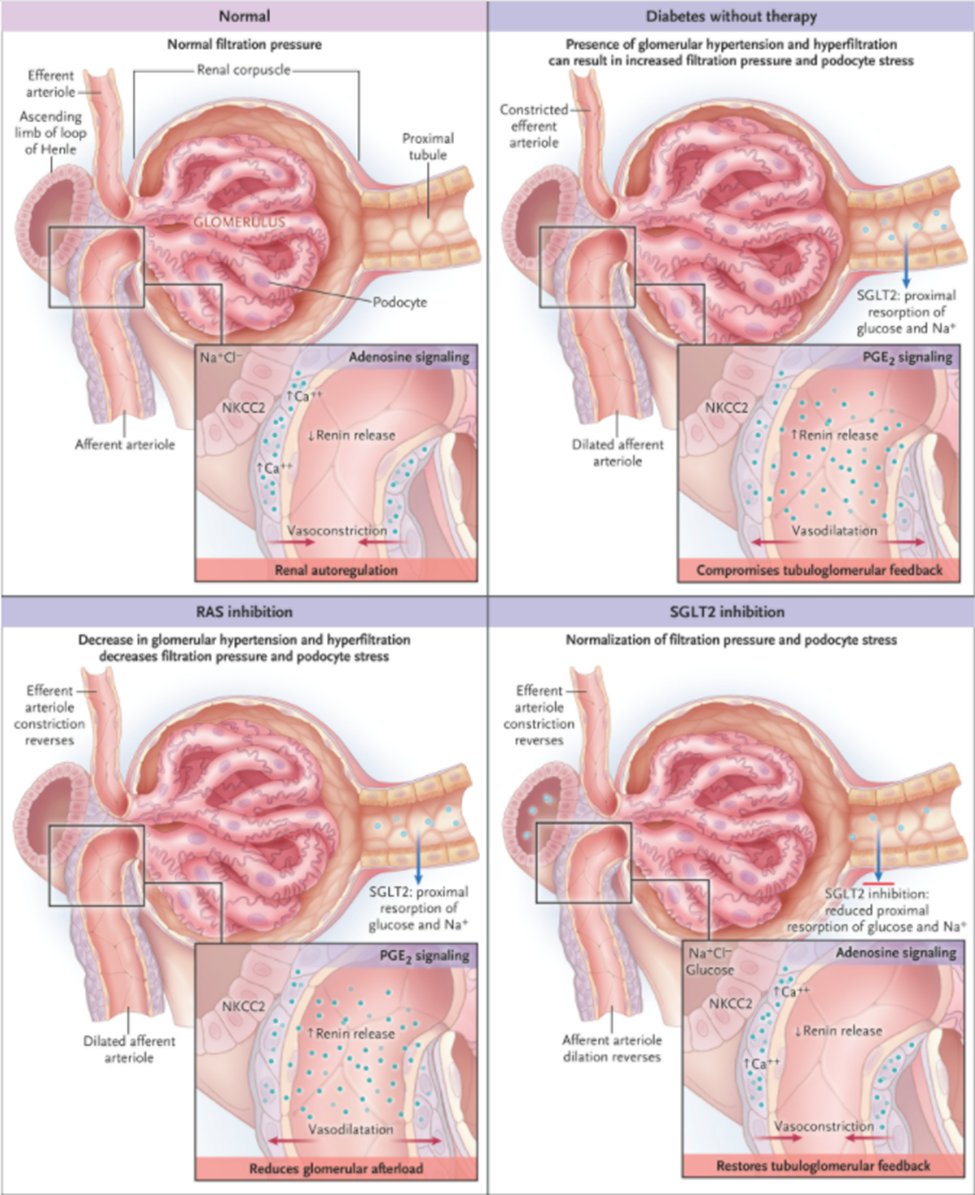
24) The most familiar renoprotective agents in #DKD that alter glomerular hemodynamics are #RAASi agents (#ACEi & #ARBs) & #SGLT2i (& there's ur answer for the❓ in tweet 19). See
nejm.org/doi/full/10.10… & for more CE/#CME on DKD tx, spend some time at ckd-ce.com/category/dkd/.
nejm.org/doi/full/10.10… & for more CE/#CME on DKD tx, spend some time at ckd-ce.com/category/dkd/.
25) For years, RAASi through ACEi and ARB have solely been relied upon as the most reliable renoprotective therapies in #DKD.
26) The emergence of SGLT2i, GLP-1 agonists and steroidal MRAs have transformed the landscape of #DKD treatment, offering new therapy options and new hope.
27) Unfortunately, achieving widespread community healthcare provider understanding of drug mechanisms, cardiac and renoprotective roles, indications for use and comfort in prescribing remains challenging.
28) SGLT2i are perhaps the best understood with the most diverse indications for use with some of the strongest supporting clinical data.
doi.org/10.1053/j.ajkd…
🔓 nephjc.com/news/dapa-ckd
doi.org/10.1053/j.ajkd…
🔓 nephjc.com/news/dapa-ckd


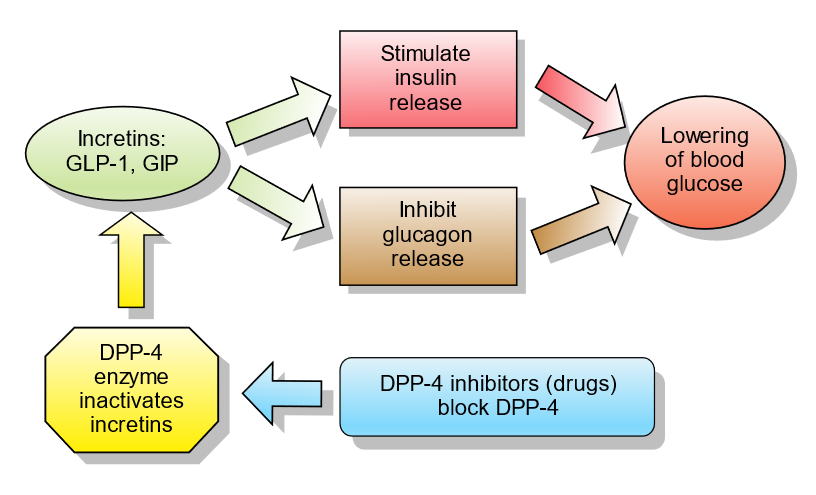
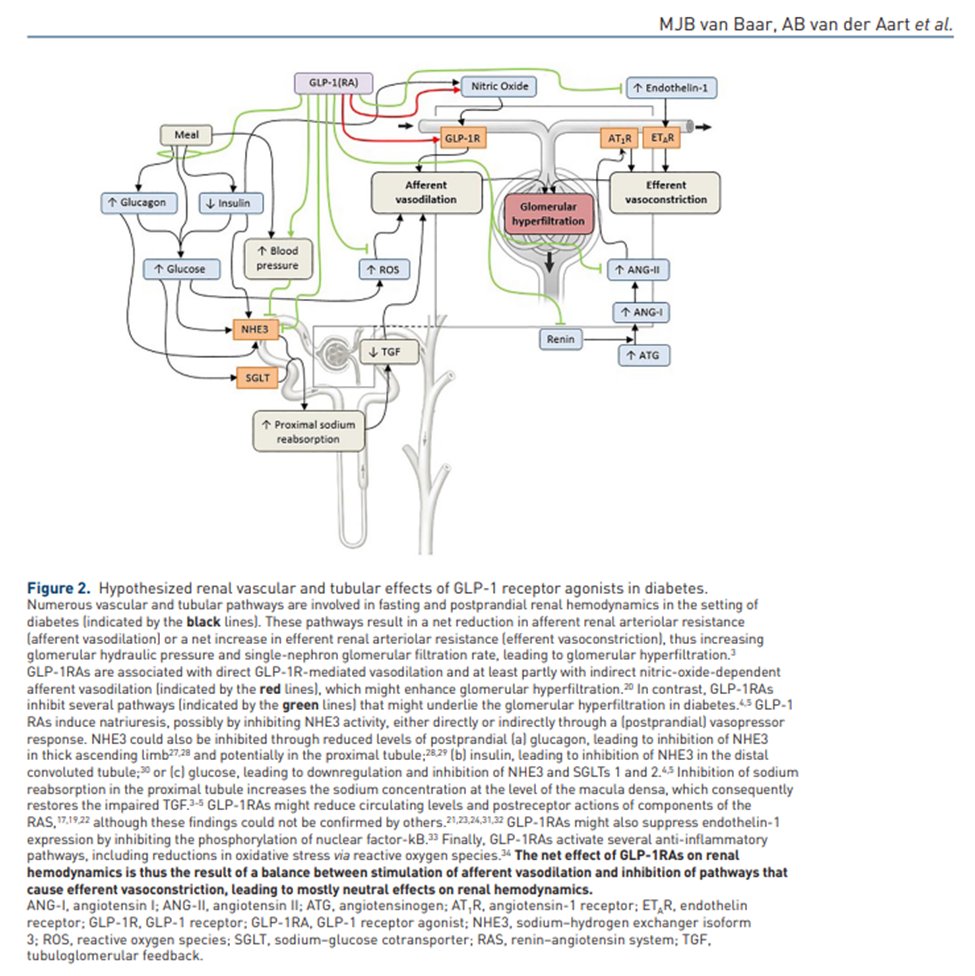
29) GLP-1 agonists are emerging as another promising #renoprotective agent with glomerular hemodynamic & anti-inflammatory/antifibrotic properties.
en.wikipedia.org/wiki/Incretin
🔓ncbi.nlm.nih.gov/pmc/articles/P…
en.wikipedia.org/wiki/Incretin
🔓ncbi.nlm.nih.gov/pmc/articles/P…
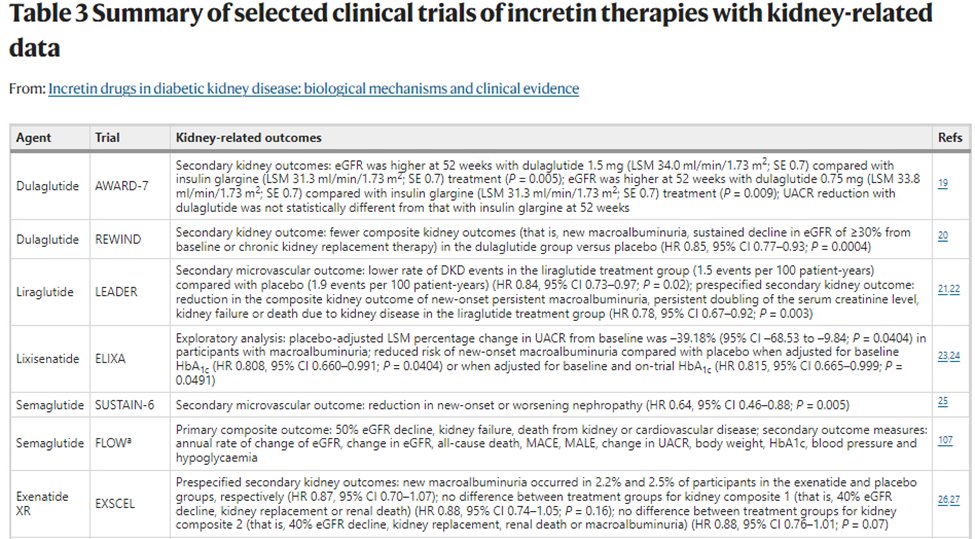
30) The GLP-1 agonist #CV outcome studies summarized below revealed mixed kidney outcome results but strongly trend towards renoprotective activity through reduction in albuminuria and/OR better secondary composite kidney outcomes
nature.com/articles/s4158…
nature.com/articles/s4158…
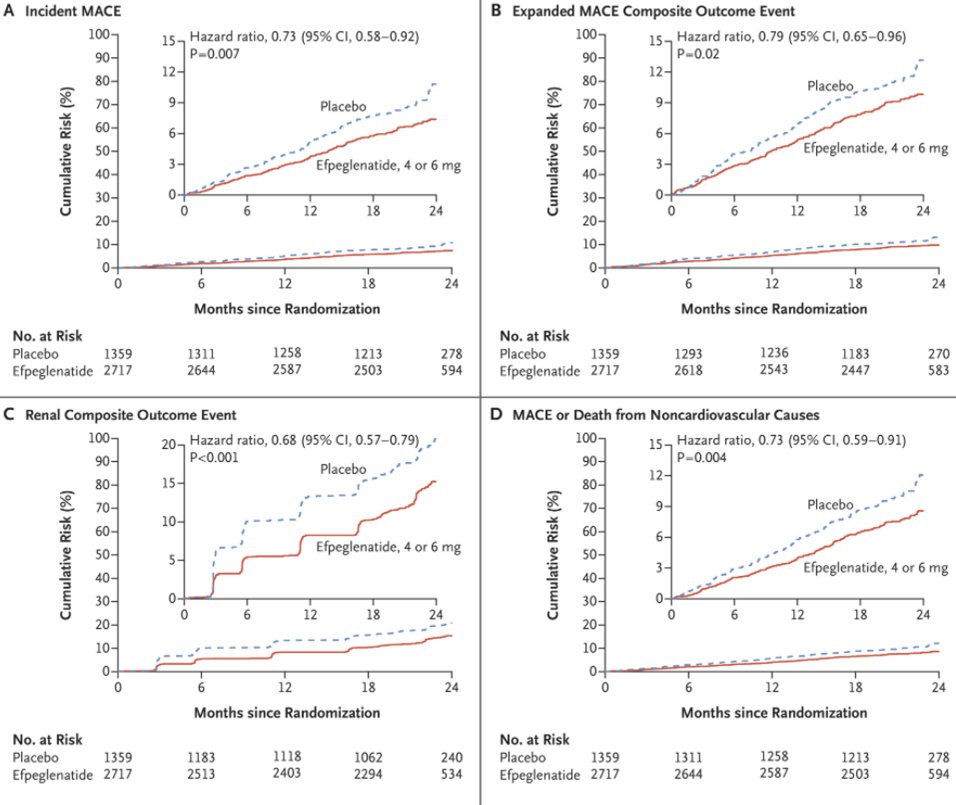
31) AMPLITUDE-O results (2021): That secondary composite renal outcome (UACR >300, UACR ≥30% increase from baseline, ESRD or death from any cause) favored efpeglenatide
🔓 nejm.org/doi/full/10.10…
🔓 nejm.org/doi/full/10.10…
32) Below are summaries of current and future clinical trials and evidence of albuminuria reduction vs GFR loss for #SGLT2i, #GLP-1 agonists (and #DPP4i).
See 🔓kdigo.org/guidelines/dia…
🔓 nephjc.com/news/dapa-ckd
See 🔓kdigo.org/guidelines/dia…
🔓 nephjc.com/news/dapa-ckd


33) Per @goKDIGO 2020 recommendations, the antihyperglycemic #T2D + #CKD algorithm (along with #RAASi, #bloodpressure mgmt & lifestyle modification) includes #metformin & #SGLT2i, and then a #GLP-1 agonist as the next preferred agent.
See 🔓kdigo.org/guidelines/dia…
See 🔓kdigo.org/guidelines/dia…

34) Let’s turn our attention to the antihypertensive therapy of mineralocorticoid receptor antagonists #MRAs
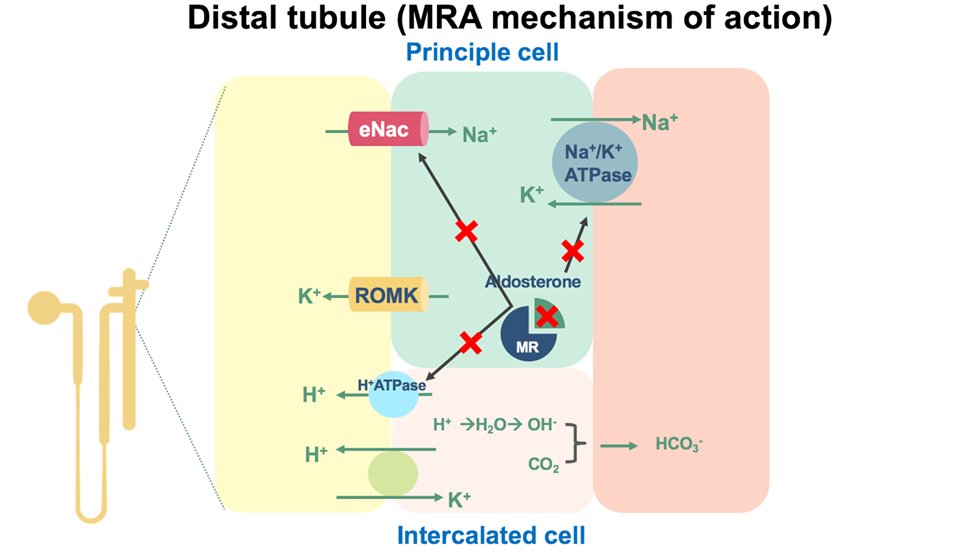
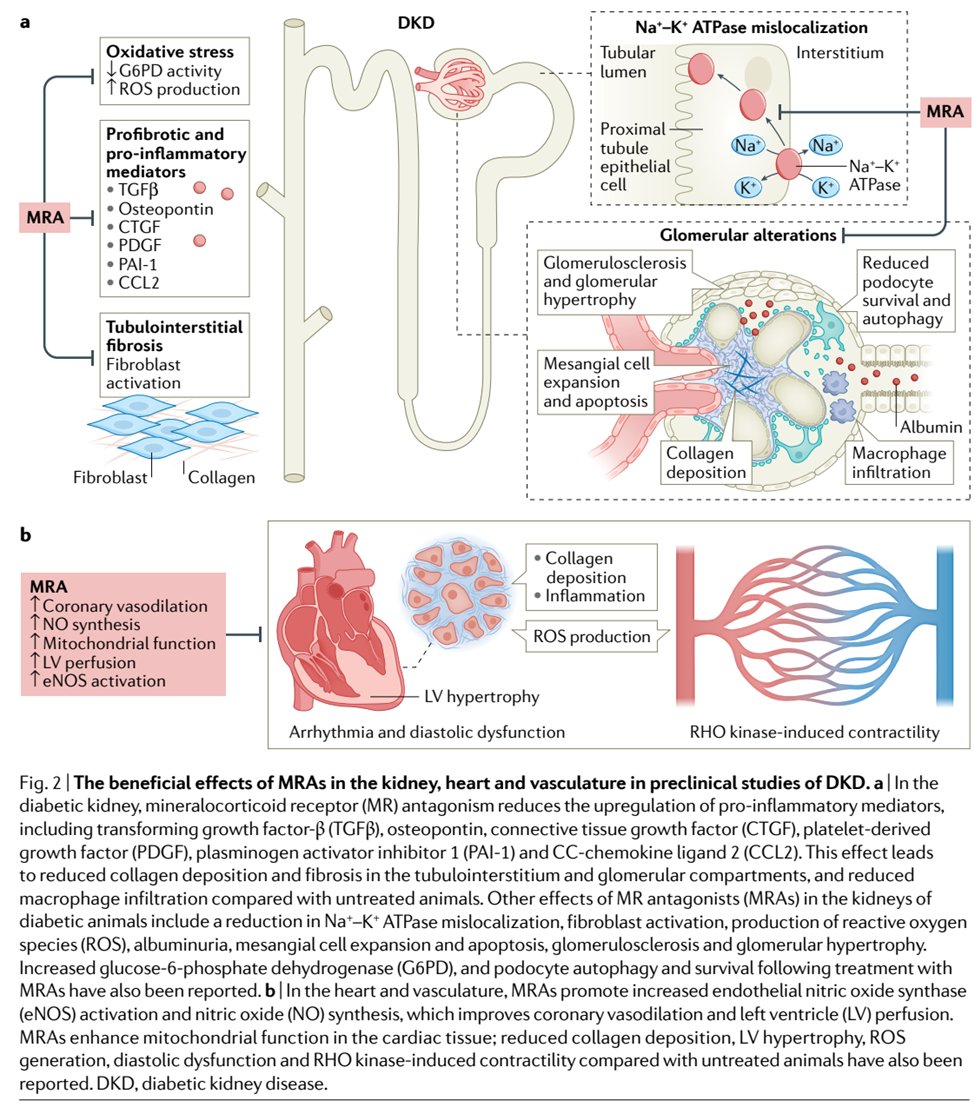
35) Preclinical data reveal #MRAs:
--reduce oxidative stress, proinflammatory mediator activity and tubulointerstitial fibrosis
--contribute to glomerular (and cardiovascular) remodeling
--⬇️ albuminuria
nature.com/articles/s4158…
--reduce oxidative stress, proinflammatory mediator activity and tubulointerstitial fibrosis
--contribute to glomerular (and cardiovascular) remodeling
--⬇️ albuminuria
nature.com/articles/s4158…
36) Preclinical models suggest more effective anti-inflammatory and antifibrotic activity w/nonsteroidal MRAs
&
The anti-androgenic & progestogenic adverse effects w/steroidal #MRAs, however less apparent with eplerenone, are suboptimal . . . and
pubmed.ncbi.nlm.nih.gov/30664703/
&
The anti-androgenic & progestogenic adverse effects w/steroidal #MRAs, however less apparent with eplerenone, are suboptimal . . . and
pubmed.ncbi.nlm.nih.gov/30664703/
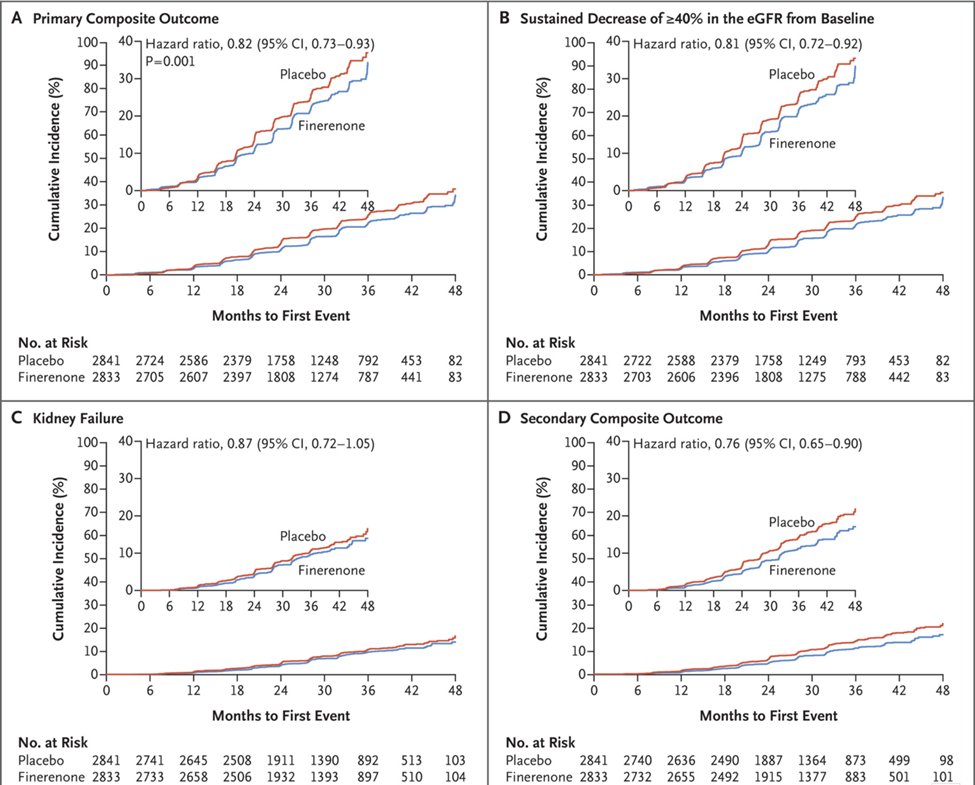
37) Clinical data w/nonsteroidal MRAs demonstrated various combinations of reduced albuminuria and/or reduction in primary composite outcome of kidney failure, sustained decrease in eGFR of 40% or more, or death of renal cause.
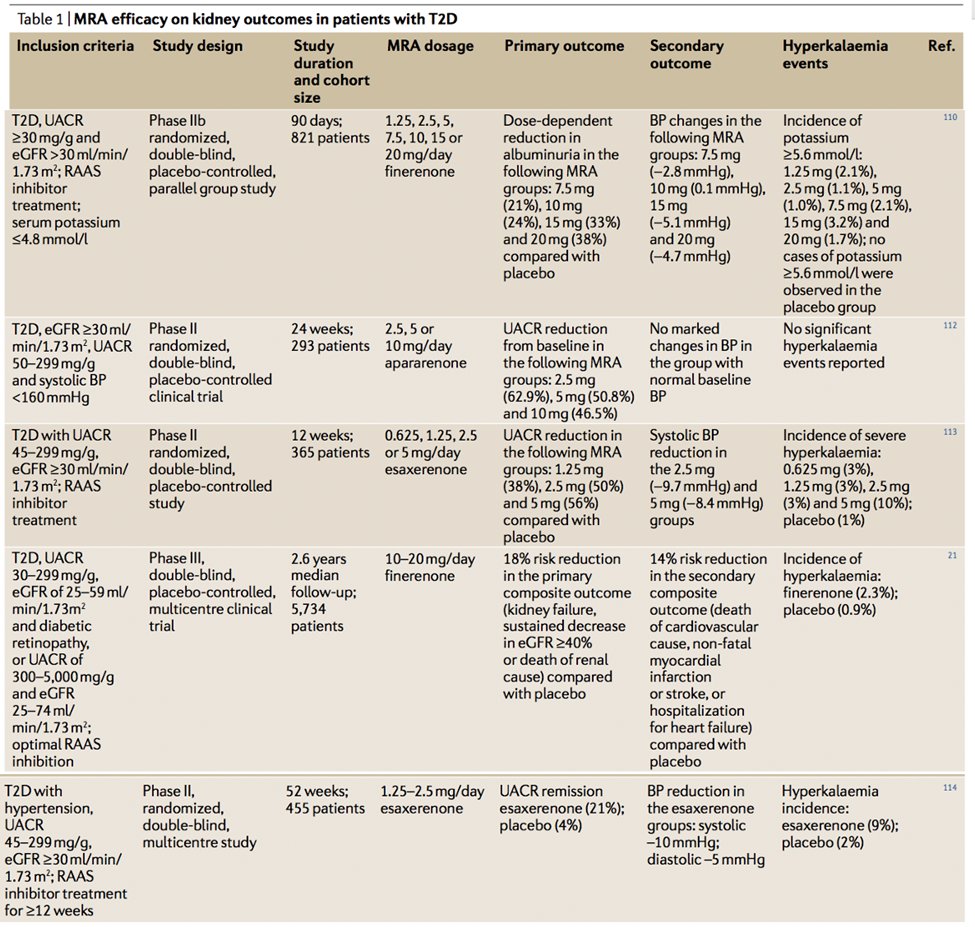
38) #FIDELIO-DKD, #RCT of finerenone vs placebo in CKD outcomes in #T2D vs placebo. Primary outcome: kidney failure, sustained eGFR decrease > 40% or death from any renal cause, N = 5674, favored finerenone, 17.8% event rate vs 21.1% w/placebo
🔓nejm.org/doi/10.1056/NE…
🔓nejm.org/doi/10.1056/NE…
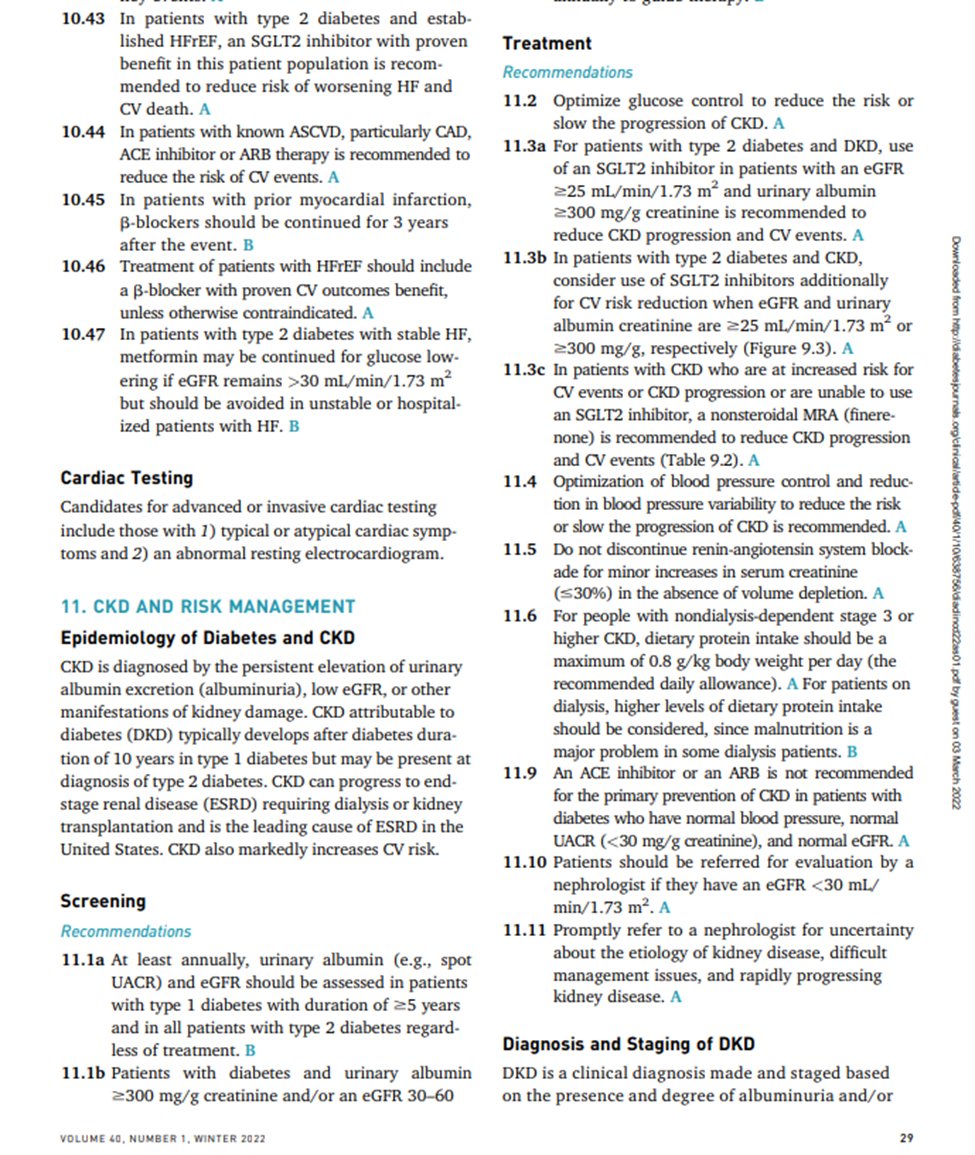
39) The American Diabetes Association @AmDiabetesAssn recommends a combination #RAASi, #SGLT2i, #GLP-1 agonists and/or nonsteroidal #MRAs (#finerenone), as guided by #UACR, serum creatinine and comorbidities.
🔓 diabetesjournals.org/clinical/artic…
🔓 diabetesjournals.org/clinical/artic…

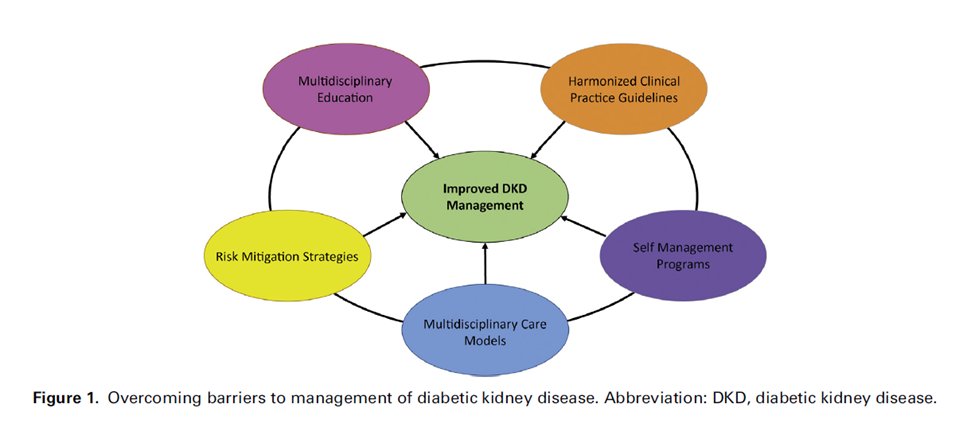
40) How to reconcile gaps in #DKD care w/new promising renoprotective medications?
Through coordinated #multidisciplinary & #interprofessional approach for early diagnosis & tx. @katherinetuttl8 @joshuaNeumiller & Dr. Alicic have outlined strategies
🔓doi.org/10.1053/j.ackd…
Through coordinated #multidisciplinary & #interprofessional approach for early diagnosis & tx. @katherinetuttl8 @joshuaNeumiller & Dr. Alicic have outlined strategies
🔓doi.org/10.1053/j.ackd…
41) We'll talk about that TOMORROW as we wrap this up & give all #physicians #physicianassociates #nurses #nursepractitioners #pharmacists a CE/#CME credit grab! Join us, @GoggleDocs @Juajal @DrPSVali @bilalksheikh @drpriyajohn @Shaque89_ @DoctorGates @kidneydoc101 @SusanQuaggin
• • •
Missing some Tweet in this thread? You can try to
force a refresh








