#FITSurvivalGuide on Restrictive Cardiomyopathy (RCM) vs Constrictive Pericarditis (CP).
In both:
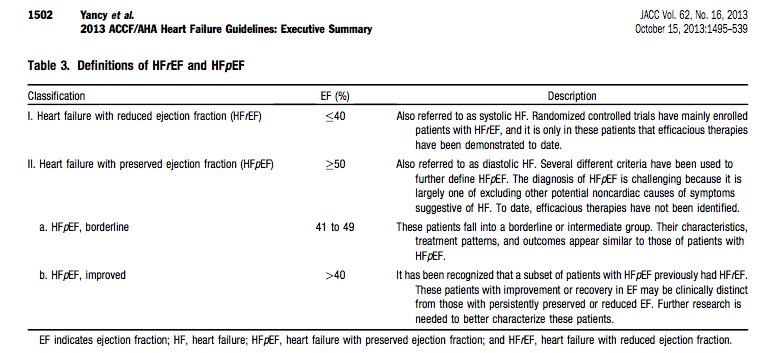
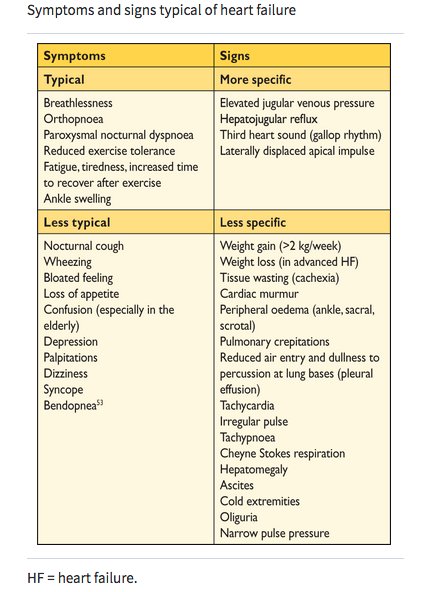
💠Diastolic RV & LV impaired; systolic function preserved
💠HFpEF phenotype, predominant “R sided” signs (JVP, edema, ascites)
1/12
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD
In both:
💠Diastolic RV & LV impaired; systolic function preserved
💠HFpEF phenotype, predominant “R sided” signs (JVP, edema, ascites)
1/12
@dr_chirumamilla @Pooh_Velagapudi @bcostelloMD
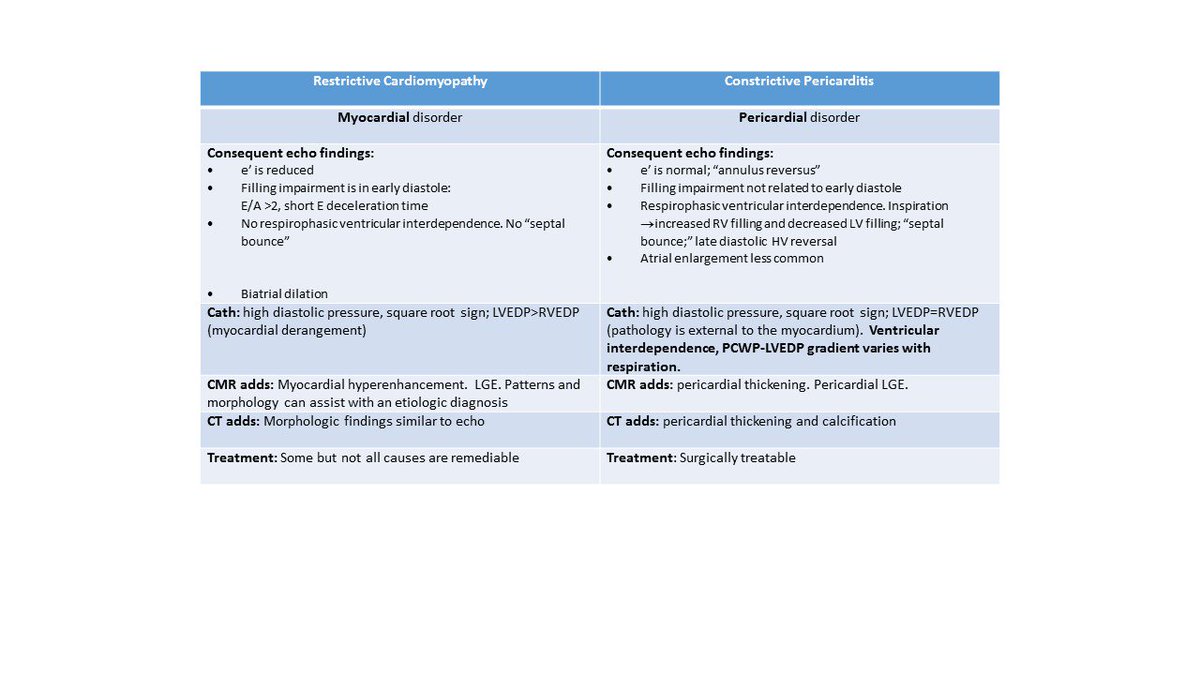
🔑 to understanding different filling:
RCM = myocardial disorder
CP = pericardial disorder.
2/12
@majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza @SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm @heartdoc45 @zainasadEP @docaward
RCM = myocardial disorder
CP = pericardial disorder.
2/12
@majazayeri @fawazalenezi55 @SanChris999 @GuruKowlgi @Nidhi_Madan9 @sabeedak1 @noshreza @SaggerMawri @nsivcd @DrManiCardio @khandelwalMD @drjohnm @heartdoc45 @zainasadEP @docaward
RCM
💠Stiff myocardium➡️early diastolic ⏫LV and RV pressure w/small vol ∆
💠 Echo: early diastolic abnormalities
💠High initial flow (= E wave; so E/A >2); ends abruptly (⬇️E decel time)
⚠️Restrictive pattern also in stage 3 HFrEF w/abnl early diastole
3/12
💠Stiff myocardium➡️early diastolic ⏫LV and RV pressure w/small vol ∆
💠 Echo: early diastolic abnormalities
💠High initial flow (= E wave; so E/A >2); ends abruptly (⬇️E decel time)
⚠️Restrictive pattern also in stage 3 HFrEF w/abnl early diastole
3/12
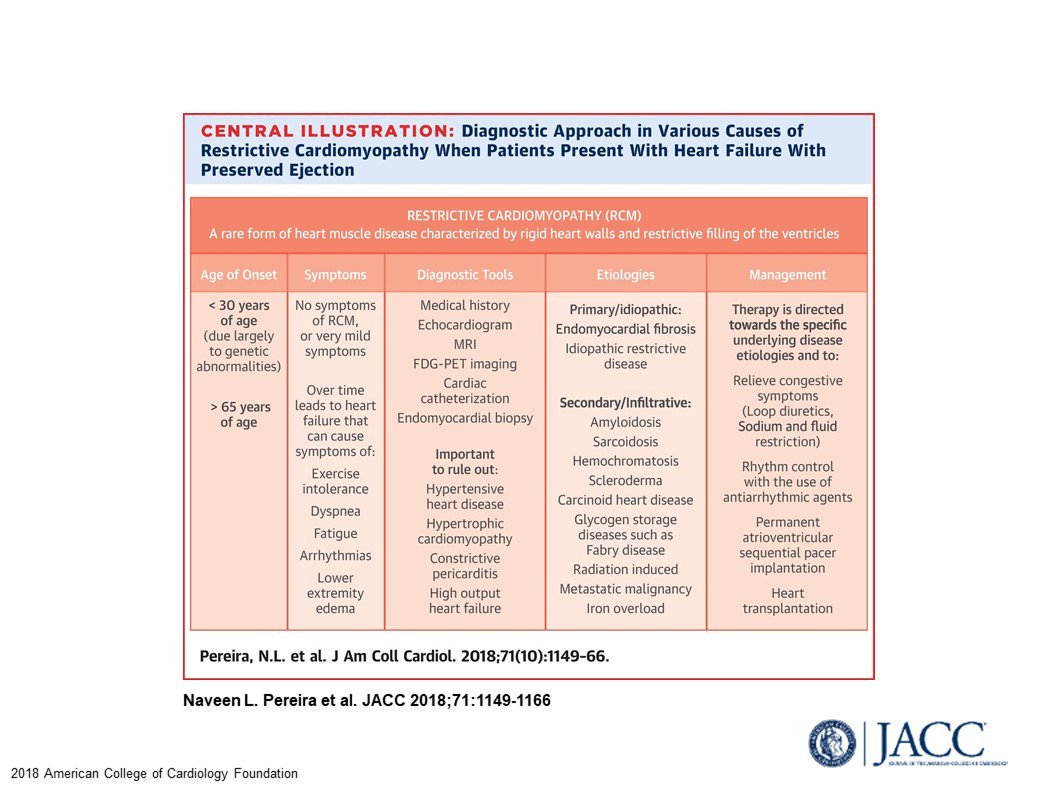
Etiologies and evaluation of RCM
4/12
@KevinShahMD @sairasamani @sarahhudsonuk @avolgman @rahatheart1 @DavidWienerMD @sunnyvmd @monsangh @feelingthepulse @achoiheart @akshitsharmaMD @adcaTicTocDoc @rezaemaminia @MartyTamMD @true_EP @onco_cardiology @sheelakrishmd @skilicmd
4/12
@KevinShahMD @sairasamani @sarahhudsonuk @avolgman @rahatheart1 @DavidWienerMD @sunnyvmd @monsangh @feelingthepulse @achoiheart @akshitsharmaMD @adcaTicTocDoc @rezaemaminia @MartyTamMD @true_EP @onco_cardiology @sheelakrishmd @skilicmd
CP
💠Pericardial shell ➡️dissociation between intrathoracic pressure (PCWP) and intracardiac (ICP) ∆s
💠Inspiration: PCWP outside the sac &⬇️; ICP inside the sac and ≠ ⬇️
💠⬇️driving gradient & LV doesn’t fill as well.
5/12
@ekgpdx @chadialraies @mirvatalasnag
💠Pericardial shell ➡️dissociation between intrathoracic pressure (PCWP) and intracardiac (ICP) ∆s
💠Inspiration: PCWP outside the sac &⬇️; ICP inside the sac and ≠ ⬇️
💠⬇️driving gradient & LV doesn’t fill as well.
5/12
@ekgpdx @chadialraies @mirvatalasnag
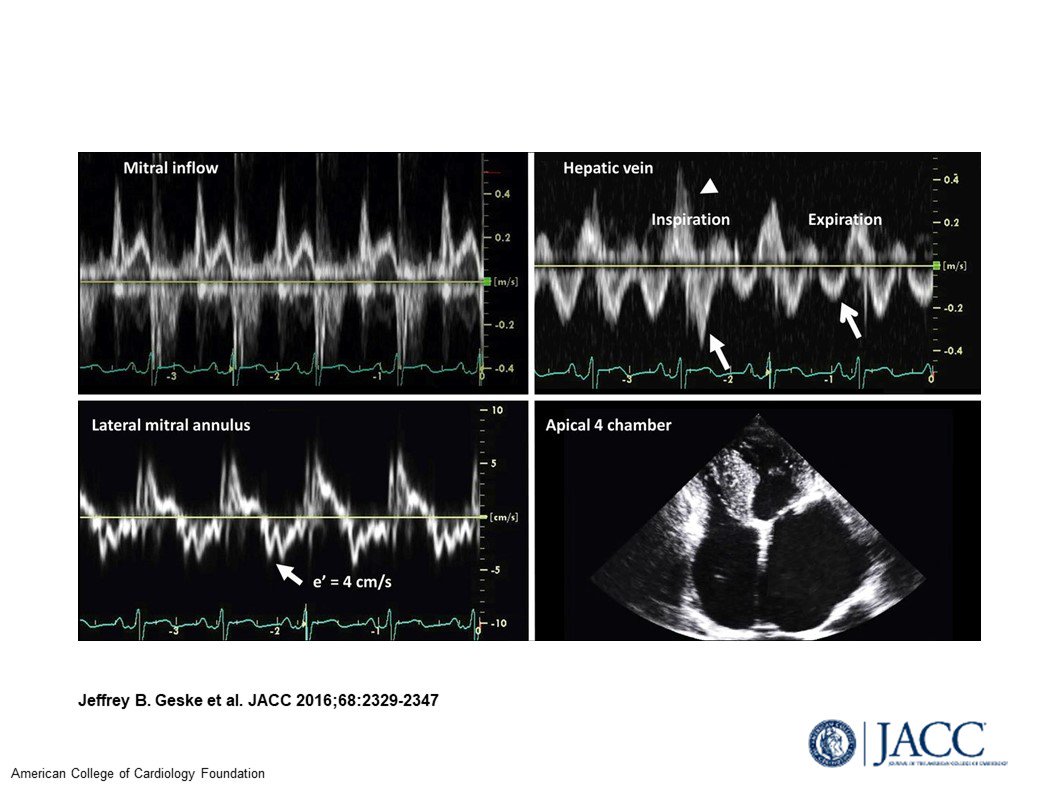
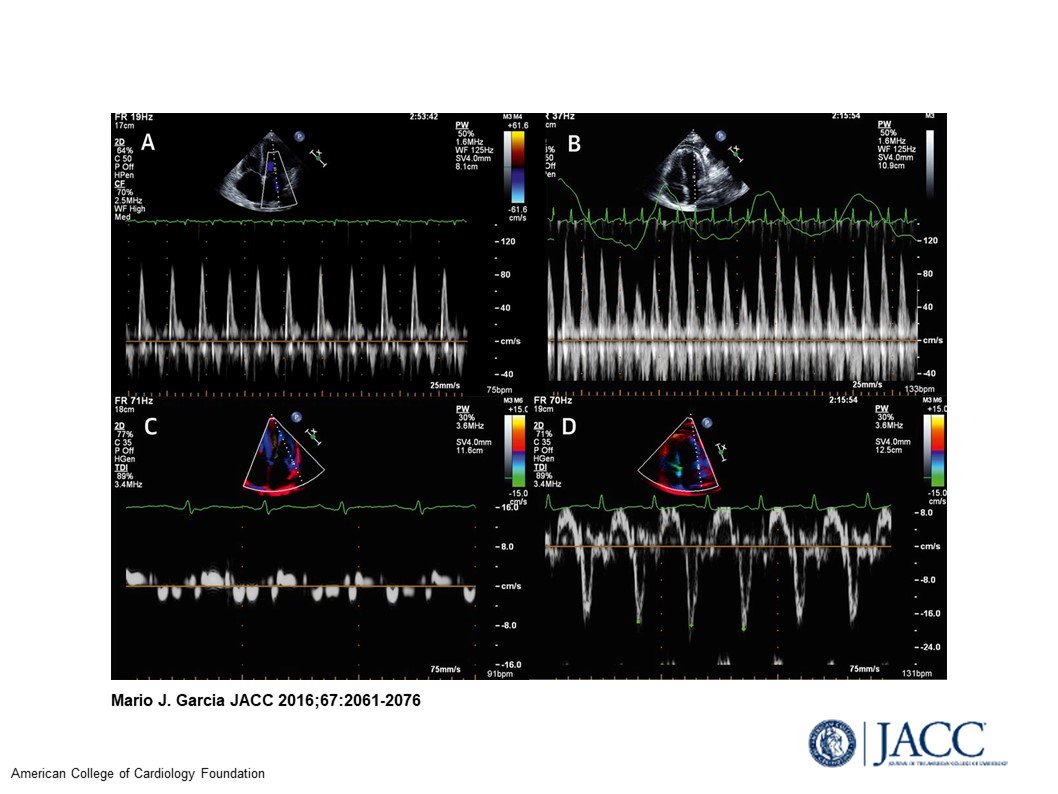
Echo in CP: exaggerated ventricular interdependence:
💠Inspiration (⬇️LV filling)
💠⬇️ MV flow
💠Septum shifts left (“bounce’ on echo)
💠RV fills better, ⬆️TV flow
💠Expiration = opposite; & HV late diastolic flow reversal (due to ⬇️RV filling)
6/12
💠Inspiration (⬇️LV filling)
💠⬇️ MV flow
💠Septum shifts left (“bounce’ on echo)
💠RV fills better, ⬆️TV flow
💠Expiration = opposite; & HV late diastolic flow reversal (due to ⬇️RV filling)
6/12

Other #EchoFirst stuff in CP
💠To dx V interdependence: turn on respirometer on machine (ask a sonographer!)
💠Other D/O also have V interdependence (tamponade)
💠Annulus reversus (lateral e’ < septal – opposite of usual). Lateral not septal
myocardium bound by pericardium
7/12
💠To dx V interdependence: turn on respirometer on machine (ask a sonographer!)
💠Other D/O also have V interdependence (tamponade)
💠Annulus reversus (lateral e’ < septal – opposite of usual). Lateral not septal
myocardium bound by pericardium
7/12
Etiologies of CP vary geographically; include
💠Idiopathic
💠Post-surgical
💠Post radiation therapy
💠Connective tissue disease
💠Neoplasia
💠Uremia
💠TB (developing countries)
8/12
@venkmurthy @fischman_david @drtoniyasingh @drmarthagulati @vietheartPA @regadenoson
💠Idiopathic
💠Post-surgical
💠Post radiation therapy
💠Connective tissue disease
💠Neoplasia
💠Uremia
💠TB (developing countries)
8/12
@venkmurthy @fischman_david @drtoniyasingh @drmarthagulati @vietheartPA @regadenoson
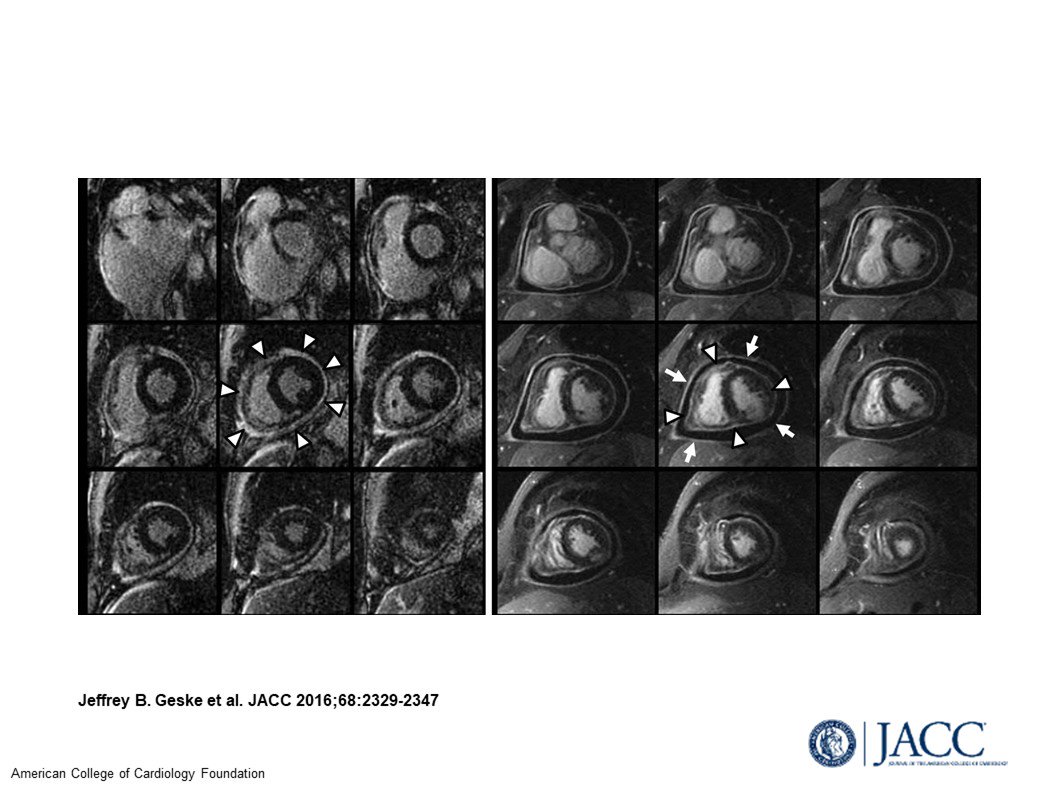
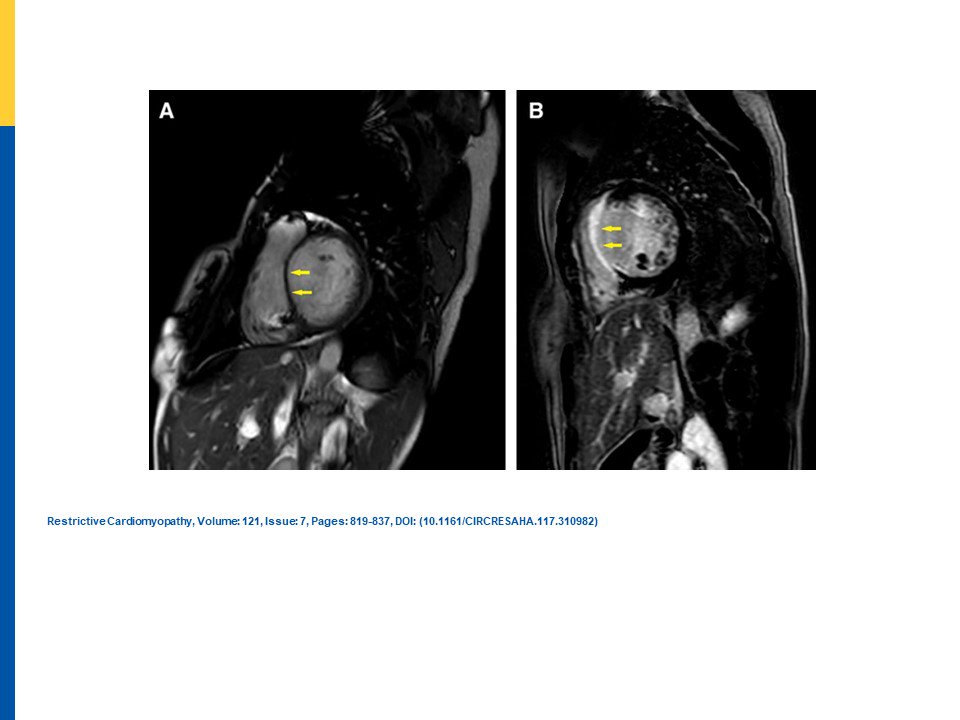
Advanced imaging helps distinguish; and helps establish etiologies (details in chart; images here!)
9/12
@cardiojaydoc02 @mark_kaeppler @mmamas1973 @CMichaelGibson @DocSavageTJU @rajivxgulati @SVRaoMD @MinnowWalsh @DrKevinCampbell @krishmd @cardiodee @DrLaxmiMehta
9/12
@cardiojaydoc02 @mark_kaeppler @mmamas1973 @CMichaelGibson @DocSavageTJU @rajivxgulati @SVRaoMD @MinnowWalsh @DrKevinCampbell @krishmd @cardiodee @DrLaxmiMehta
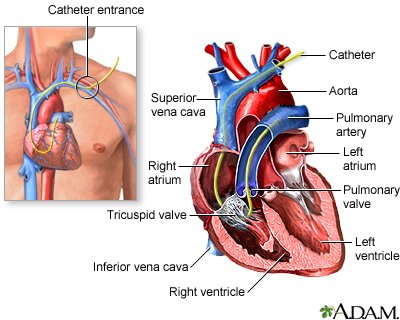
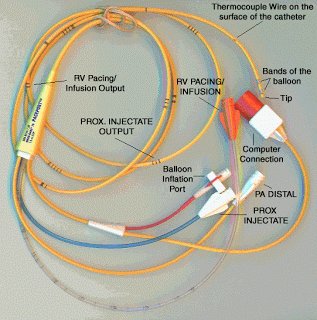
Cath
💠Both: early rapid filling, square root sign.
💠“Classic” criteria to distinguish (= pressures, ⬆️RVSP, LVEDP>RVEDP) are < specific than thought
🔑 for CP: RV vs LV filling varies with respiration. PCWP-LVP gradient varies by >5 mm with respiration
10/12
💠Both: early rapid filling, square root sign.
💠“Classic” criteria to distinguish (= pressures, ⬆️RVSP, LVEDP>RVEDP) are < specific than thought
🔑 for CP: RV vs LV filling varies with respiration. PCWP-LVP gradient varies by >5 mm with respiration
10/12

References and Summary Table:
JACC 2016;68:2329–47
JACC 2016;67:2061–76
Circ Res 2017;121:819-837
J Am Coll Cardiol 2018;71:1149–66
Am Coll Cardiol 2018;71:1130–48
Cath and multimodality colleagues: input invited! 😉
11/12
@ash71us @purviparwani @gina_lundberg
JACC 2016;68:2329–47
JACC 2016;67:2061–76
Circ Res 2017;121:819-837
J Am Coll Cardiol 2018;71:1149–66
Am Coll Cardiol 2018;71:1130–48
Cath and multimodality colleagues: input invited! 😉
11/12
@ash71us @purviparwani @gina_lundberg