Our #FITSurvivalGuide continues with antiarrhythmic drugs! (AADs)
1️⃣Basic concepts
2️⃣Classification
3️⃣Class 1(a/b/c)
4️⃣Class 3
5️⃣Amio/dronedarone
6️⃣Clinical use
7️⃣Pearls and pitfalls
1️⃣Basic concepts
2️⃣Classification
3️⃣Class 1(a/b/c)
4️⃣Class 3
5️⃣Amio/dronedarone
6️⃣Clinical use
7️⃣Pearls and pitfalls

1️⃣ Arrhythmias originate from ectopy +/- reentry.
AADs work by:
*⬇️ing ectopy
*⬆️ing refractoriness (⬇️ing reentry)
AADs work by:
*⬇️ing ectopy
*⬆️ing refractoriness (⬇️ing reentry)
2️⃣
Class1: sodium channel blockers
(⬇️ ectopy, ⬇️ reentry by raising threshold for cell-cell conduction)
C2: beta blockers
C3: potassium channel blockers
(⬆️ action potential, ⬆️ AP "wavelength", ⬇️ excitable gap for reentry)
C4: calcium channel blockers
Class1: sodium channel blockers
(⬇️ ectopy, ⬇️ reentry by raising threshold for cell-cell conduction)
C2: beta blockers
C3: potassium channel blockers
(⬆️ action potential, ⬆️ AP "wavelength", ⬇️ excitable gap for reentry)
C4: calcium channel blockers
3️⃣Class1- mnemonic for subclasses
1a Double Quarter Pounder
Disopyramide
Quinidine
Procainamide
1b Lettuce Mayo Tomato
Lidocaine
Mexiletine
Tocainide
1c More Fries Please!
Moricizine
Flecainide
Propafenone
1a Double Quarter Pounder
Disopyramide
Quinidine
Procainamide
1b Lettuce Mayo Tomato
Lidocaine
Mexiletine
Tocainide
1c More Fries Please!
Moricizine
Flecainide
Propafenone
3️⃣ Class1 drugs are USE DEPENDENT: bind to active form of Na channel.
Faster heart rates, depolarized (ischemic) tissues result in greater effect.
Faster heart rates, depolarized (ischemic) tissues result in greater effect.

3️⃣Class 1a- moderate Na blockers, ⬆️QT!
Specialized use:
Disopyramide- AF+HCM
Quinidine- VF in BrugadaSy
Procainamide- IV only- acute Tx for preexcited AF, VT/VF esp planning ablation (shorter t1/2 than amio). NAPA= proc metabolite that ⬆️ QT, careful with kidney failure!
Specialized use:
Disopyramide- AF+HCM
Quinidine- VF in BrugadaSy
Procainamide- IV only- acute Tx for preexcited AF, VT/VF esp planning ablation (shorter t1/2 than amio). NAPA= proc metabolite that ⬆️ QT, careful with kidney failure!
3️⃣ Class 1b- weak Na channel blockers. Best use in ischemic arrhythmias or when contraindications to all others.
Lidocaine IV, mexiletine PO.
Side effects of AV block, tremors➡️seizures. Careful with CHF or liver failure!
Take mexiletine with food to avoid nausea.
Lidocaine IV, mexiletine PO.
Side effects of AV block, tremors➡️seizures. Careful with CHF or liver failure!
Take mexiletine with food to avoid nausea.
3️⃣Class 1c- strong Na blockers. Good for focal tachycardias (nonreentrant AT, idiopathic PVCs/VT) as well as AFib.
Risk of "organizing" AFib to slow AFL with 1:1 conduction!
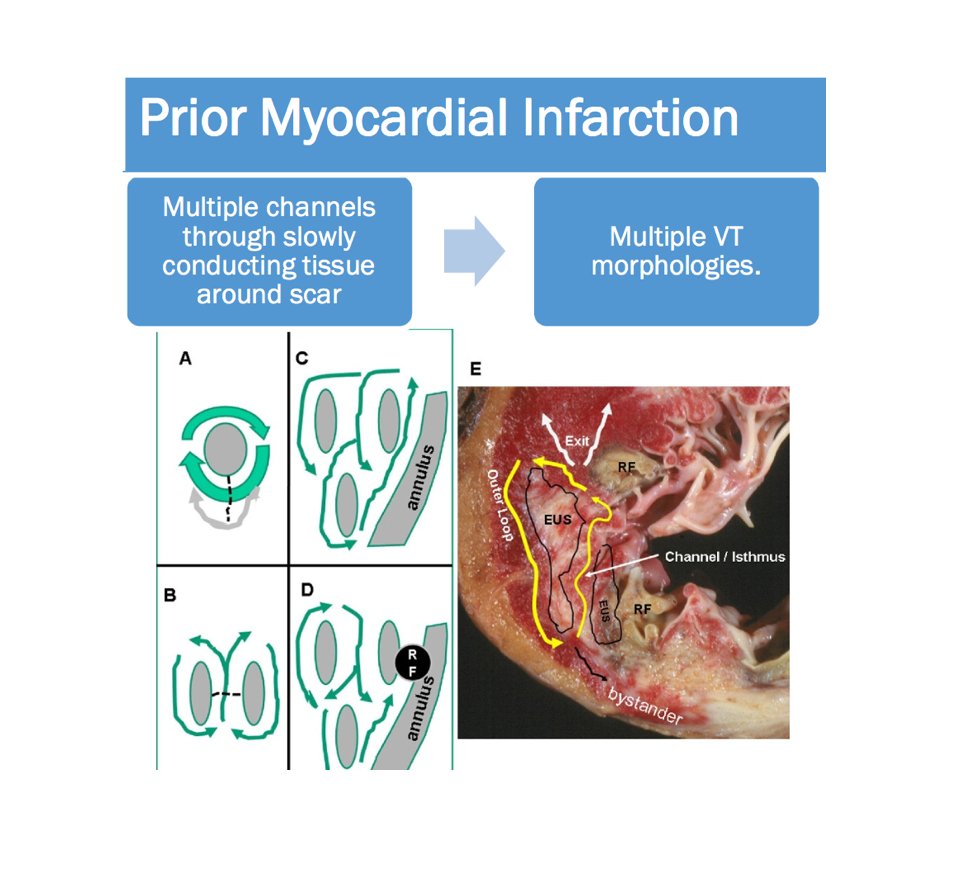
Risk of sudden death in structural heart disease (primarily MI but any ventricular scar prob applies)
Risk of "organizing" AFib to slow AFL with 1:1 conduction!
Risk of sudden death in structural heart disease (primarily MI but any ventricular scar prob applies)
4️⃣ Class 3. Potassium channel blockers.
Prolong QT by definition, risk of torsades.
REVERSE USE DEPENDENT: greater effect in bradycardia!
Much like other QT⬆️ing Rx and LQTS, brady = danger!
Renally cleared.
Prolong QT by definition, risk of torsades.
REVERSE USE DEPENDENT: greater effect in bradycardia!
Much like other QT⬆️ing Rx and LQTS, brady = danger!
Renally cleared.
4️⃣ Sotalol: nonselective Bb and K antagonist.
Bb action can cause bronchospasm, fatigue. Inpatient initiation due to ⬆️QT.
Useful for AF, substrate-mediated VT (ischemic scar, ARVC, sarcoid et al)
Bb action can cause bronchospasm, fatigue. Inpatient initiation due to ⬆️QT.
Useful for AF, substrate-mediated VT (ischemic scar, ARVC, sarcoid et al)
4️⃣ Ibutilide: IV only. STRONG anti-K, risk of torsades, given under direct supervision.
Useful for:
*chemical cardioversion of AF
*pre-excited AF
*recurrent AT/AF post cardioversion
Useful for:
*chemical cardioversion of AF
*pre-excited AF
*recurrent AT/AF post cardioversion
4️⃣ Dofetilide: strong anti-K, PO version.
Only for AFib/AT.
MUST be careful with initiation. No longer need to register to prescribe, but FOLLOW INITIATION GUIDELINES!
Only for AFib/AT.
MUST be careful with initiation. No longer need to register to prescribe, but FOLLOW INITIATION GUIDELINES!

5️⃣ Amiodarone: best and worst AAD.
Pros: most effective drug for AF/AT, VT/VF.
Cons: pulmonary fibrosis, hepatitis, hypothyroid (can supplement), hyperthyroid (usually have to stop), corneal deposits, optic neritis, large muscle weakness dt neuropathy.
Pros: most effective drug for AF/AT, VT/VF.
Cons: pulmonary fibrosis, hepatitis, hypothyroid (can supplement), hyperthyroid (usually have to stop), corneal deposits, optic neritis, large muscle weakness dt neuropathy.

5️⃣ Dronedarone: worst and best AAD.
Cons: weakest AAD. Limited use for AFib/AT which is easy to control. Risk of sudden death with CHF.
Pros: minimal long term side effects, easy to use (no load, no ischemic wu prior to start).
Can cause diarrhea, may Rx with immodium.
Cons: weakest AAD. Limited use for AFib/AT which is easy to control. Risk of sudden death with CHF.
Pros: minimal long term side effects, easy to use (no load, no ischemic wu prior to start).
Can cause diarrhea, may Rx with immodium.
6️⃣Contraindications= KEY to AAD use!
Structural heart disease 🚫1c
LBBB/RBBB/hemiblock 🚫1a/b/c
Sinus brady🚫all, esp sotalol/amio/dron
Renal failure🚫3
QT ⬆️ing Rx🚫3, 1a
Liver failure 🚫1b/amio/dron
CHF🚫1b,1c
LOTS OF INTERACTIONS!
DOACs, Abx, psych Rx, chemo common
Structural heart disease 🚫1c
LBBB/RBBB/hemiblock 🚫1a/b/c
Sinus brady🚫all, esp sotalol/amio/dron
Renal failure🚫3
QT ⬆️ing Rx🚫3, 1a
Liver failure 🚫1b/amio/dron
CHF🚫1b,1c
LOTS OF INTERACTIONS!
DOACs, Abx, psych Rx, chemo common
6️⃣ AFib/AT:
1c if no CAD/CHF/conduction diz
3 if no renal failure and no QT interactions
Dron if early AF, prefer easy-to-start Rx
Amio if advanced AF, older pt, younger pt for TRIAL of Tx
PRE-EXCITED AFIB:
procainamide or ibutilide, avoid AVN blockers!
1c if no CAD/CHF/conduction diz
3 if no renal failure and no QT interactions
Dron if early AF, prefer easy-to-start Rx
Amio if advanced AF, older pt, younger pt for TRIAL of Tx
PRE-EXCITED AFIB:
procainamide or ibutilide, avoid AVN blockers!
6️⃣ PVCs/idiopathic VT:
1c if no structural ht diz
1c if no structural ht diz
6️⃣Structural VT
Amio acutely, older/sicker pts, young pts failing other Tx
Procainamide acute, BRIDGE TO ABLATION
Lido acute ischemic VT
Sotalol ischemic-substrate VT
Quinidine Brugada
Flecainide CPVT
Sotalol/amio ARVC
Mexiletine low-risk option when others contraindicated
Amio acutely, older/sicker pts, young pts failing other Tx
Procainamide acute, BRIDGE TO ABLATION
Lido acute ischemic VT
Sotalol ischemic-substrate VT
Quinidine Brugada
Flecainide CPVT
Sotalol/amio ARVC
Mexiletine low-risk option when others contraindicated
7️⃣Pearls and pitfalls:
MOST AAD HAVE ⬛️ WARNING
All cause sinus brady to some extent
Most proarrhythmic
Consider pros/cons in each pt
Don't forget non-drug options (cardioversion acutely, ablation electively)
MOST AAD HAVE ⬛️ WARNING
All cause sinus brady to some extent
Most proarrhythmic
Consider pros/cons in each pt
Don't forget non-drug options (cardioversion acutely, ablation electively)
7️⃣Inpt drug initiation:
9am/9pm dose with 11am/11pm ECG
Allows reasonable timing of dose/ECG, and YOU CAN STILL INTERCEPT THE AM DOSE THE NEXT MORNING without having to look up ECGs at midnight! 😉
CHECK THE TELE, don't just assume a normal QT means no torsades 🤦🏻♂️
9am/9pm dose with 11am/11pm ECG
Allows reasonable timing of dose/ECG, and YOU CAN STILL INTERCEPT THE AM DOSE THE NEXT MORNING without having to look up ECGs at midnight! 😉
CHECK THE TELE, don't just assume a normal QT means no torsades 🤦🏻♂️
7️⃣ Long term...
Class 1a/b/c: ECG q6M (look for intraventricular blocks)
Class 3: ECG q6M, renal function q12M (look for QT prolongation)
Amio: ECG, LFTs, TSH/T4, CXR q6M ➡️q12M
Dron: ECG, LFTs q6M➡️q12M
Class 1a/b/c: ECG q6M (look for intraventricular blocks)
Class 3: ECG q6M, renal function q12M (look for QT prolongation)
Amio: ECG, LFTs, TSH/T4, CXR q6M ➡️q12M
Dron: ECG, LFTs q6M➡️q12M
And finally, THE DISCLAIMER:
This is by no means EVERYTHING you'll need to know in order to use AADs. These are just a few pearls to get started. When in doubt, CALL YOUR ATTENDING before starting AAD, because it can have major side effects and interfere with ablation plans!
This is by no means EVERYTHING you'll need to know in order to use AADs. These are just a few pearls to get started. When in doubt, CALL YOUR ATTENDING before starting AAD, because it can have major side effects and interfere with ablation plans!
I just realized (AND NO ONE CALLED ME OUT!) 😅🤦🏻♂️ that I left out Dronedarone contraindicated in CHF.