,
27 tweets,
6 min read
Read on Twitter
Warning! Tweetorial Ahead:
I was consulted for hyponatremia.
The sodium was 122 and the patient was apparently asymptomatic.
I was consulted for hyponatremia.
The sodium was 122 and the patient was apparently asymptomatic.
First step:
A. We’re in the ER, so a liter of NS
B. Check serum osmolality
C. Careful exam to categorize the patient’s volume status
A. We’re in the ER, so a liter of NS
B. Check serum osmolality
C. Careful exam to categorize the patient’s volume status
The next step is to check osmolality (A) to confirm we are dealing with hypo-osmotic hyponatremia. By the way, the patient was in the ER so they did get the obligatory liter of NS.
The patient had an excellent ER doc who did a complete biochemical assessment of hyponatremia:
Serum osmolality 303
Urine osmolality 103
Urine Na < 20
Urine K 6
Serum osmolality 303
Urine osmolality 103
Urine Na < 20
Urine K 6
So one of these labs is not like the other, which is it?
A. Serum osmolality should be low
B. Urine osmolality should be high due to the kidney retaining water
C. The urine Na is low, patients with hyponatremia should not be retaining Na.
D. Where’s my uric acid!
A. Serum osmolality should be low
B. Urine osmolality should be high due to the kidney retaining water
C. The urine Na is low, patients with hyponatremia should not be retaining Na.
D. Where’s my uric acid!
The serum osmolality is the right answer again. The high plasma osmolality with a low plasma sodium is a weird situation that should derail you from standard hyponatremia algorithm 
In my standard hyponatremia teaching I categorize hyponatremia with a normal or high osmolality as false hyponatremia. That is not the whole story.

Hyponatremia with a normal osmolality should make you think of pseudohyponatremia due to excess lipids or serum protein causing a lab artifact (if your lab still indirect ion selective electrodes (ISE). Most labs are not susceptible to this artifact because they use direct ISE)
There is another unusual cause of this combination of low sodium and normal osmolality. This is during prostatic surgery when the surgeons use 5% mannitol as irrigation and excess is absorbed into the circulation. ncbi.nlm.nih.gov/pmc/articles/P…
The mannitol is isotonic, osmolality 275. The mannitol dilutes the sodium, but the osmolality of the body does not change. If the complication occurs with hypotonic irrigation fluids (1.5% Glycine, osmolality 200 or 3% sorbitol, osmolality 165) then the Na and osmolality falls.
Nice reference of TURP syndrome: ncbi.nlm.nih.gov/pmc/articles/P…
Hyponatremia with a high osmolality means there is an additional solute besides sodium in the extracellular compartment. These can be osmotically active or osmotically inactive.
The more interesting ones are the ones that are osmotically active, like glucose or mannitol. They are interesting because they cause both the hyperosmolality and the hyponatremia.
Hyponatremia with increased osmolality is classically seen with hyperglycemia. Here the the increased extracellular glucose is osmotically active so it draws water from the intracellular compartment which then dilutes the extracellular sodium. So you have ↓Na and ↑osmolality
Since these patients are hypertonic they will behave more like patients with hypernatremia, expressing increased thirst and concentrating their urine in order to retain free water to lower serum osmolality.
In addition to glucose, you can also see this with mannitol.
onlinelibrary.wiley.com/doi/full/10.11…
onlinelibrary.wiley.com/doi/full/10.11…
So in my patient I checked the serum glucose, 80 mg/dL and did a thorough review of systems that confirmed to me that he had not received any mannitol in the recent past.
There may be other osmotically active solutes that cause hypertonic hyponatremia but I can’t think of any. (Please @ me if you have one)
So that leaves the actual diagnosis, the patient had hyponatremia with an excess of an osmotically inactive solute. This can be seen with ethanol or BUN (kidney failure) (BUN).
Since ethanol and BUN diffuse across the cell membrane (they osmotically inactive) they do not cause water to move out of the cell (the hall mark of true hypotonic hyponatremia).
The elevated osmolality is also not the cause of the hypontremia and the hyponatremia still has to be diagnosed and treated in the usual way.
The best article on this is
The best article on this is
So we explained the elevated osmolality, but that doesn't explain the hyponatremia which still needs to be diagnosed and treated. This is different from hyponatremia with elevated osmolality from an osmotically active solute, where you should focus on treating the hyperosmolality
Looking at the labs what do you think the diagnosis is?
Serum osmolality 303
Urine osmolality 103
Urine Na < 20
Urine K 6
Serum osmolality 303
Urine osmolality 103
Urine Na < 20
Urine K 6
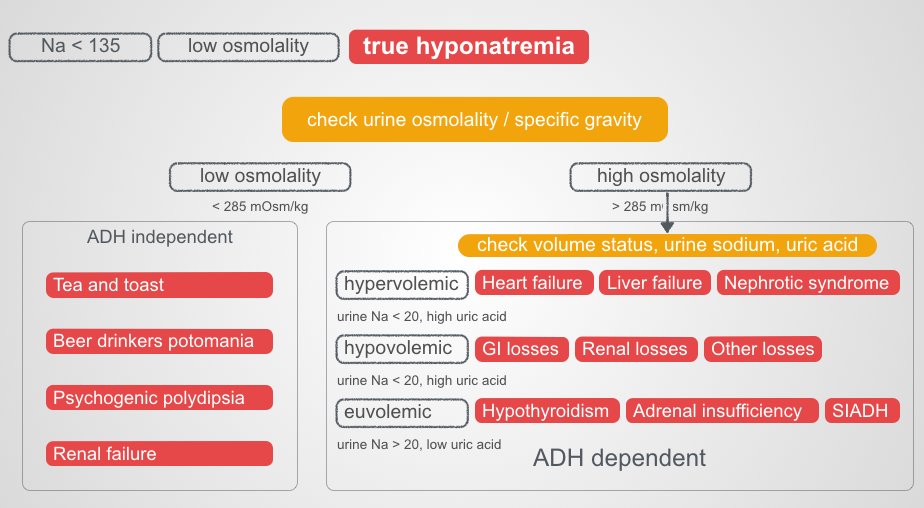
Look at the urine osmolality. It is low Look to the ADH independent causes of hyponatremia.

This was the diagnosis. The patient had been on a beer only bender for weeks and had no essentially no other nutrition.
Fin.
Fin.