
Over the past two days we've covered math of exponential growth and epidemics. Today we'll talk about the new Imperial College of London report "Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand"
The report is based on an individual-based model published in 2005 and 2006 papers in Nature. "Strategies for containing an emerging influenza pandemic in SE Asia" and "Strategies for mitigating an influenza pandemic"
imperial.ac.uk/media/imperial…
imperial.ac.uk/media/imperial…
It's very hard to track down the methods because the report links to the 2006 paper with methods in the supporting information, which itself links to the supporting information of the 2005 paper. The model incorporates an incredible amount of detail. Such as...
Population density data, household size and age structure, school size and location, distribution of workplace size and location, and travel data (needed for spread). An individual in the model is defined by their age, household, and place.
Individuals are co-located in households, with households being constructed to reflect typical generational structure while matching empirical distributions of age structure and household size. They discriminate between place types including schools and workplaces.
The proportions of individuals attending different place types varied by age, and they assumed individuals
are members of only one place. Places are distributed randomly in space, with a density proportional to that of the population.
are members of only one place. Places are distributed randomly in space, with a density proportional to that of the population.
Because this was an individual based model, they were able to assess the following policy options. Case isolation in the home. Voluntary home quarantine. Social distancing of those >70yrs old. Social distancing of everyone. School and university closure.
They assume R0=2.4 based on the data from Wuhan. Without intervention, they predict 80% of US and UK population are infected and 2.2 million and 510,000 deaths in US and UK. Note that this 80% infected is very similar to the result from the model with R0=2.5 from yesterday.
Without any intervention they "predict critical care bed capacity would be exceeded as early as the second week in April, with an eventual peak in ICU or critical care bed demand that is over 30 times greater than the maximum supply in both countries." Intervention helps a bit... 

"Stopping mass gatherings is predicted to have relatively little impact (results not shown) because the contact-time at such events is relatively small compared to the time spent at home, in schools or workplaces and in other community locations such as bars and restaurants."
"Overall, we find that the relative effectiveness of different policies is insensitive to the choice of local trigger (absolute numbers of cases compared to per-capita incidence), R0 (in the range 2.0-2.6), and varying IFR in the 0.25%-1.0% range."
The take home is that mitigation fails and we need to be talking about suppression. "to reduce R to close to 1 or below, a combination of case isolation, social distancing of the entire population and either household quarantine or school and university closure are required "

"Once interventions are relaxed, infections begin
to rise, resulting in a predicted peak epidemic later in the year. The more successful a strategy is at temporary suppression, the larger the later epidemic is predicted to be in the absence of vaccination"
to rise, resulting in a predicted peak epidemic later in the year. The more successful a strategy is at temporary suppression, the larger the later epidemic is predicted to be in the absence of vaccination"
Individual based models are impossible to get "right" and it's hard to give them robust peer review. There are so many moving parts. They do a sensitivity analysis to see how results vary with uncertainty around the parameters, but this uncertainty isn't propagated.
In the 2006 paper "In any time-step of ΔT=0.25 days, a susceptible individual i has probability 1−exp(−λ_iΔT) of being infected, where λ_i is the instantaneous infection risk for individual i." The expression for λ_i is given in the 2005 paper only and it's a beast.
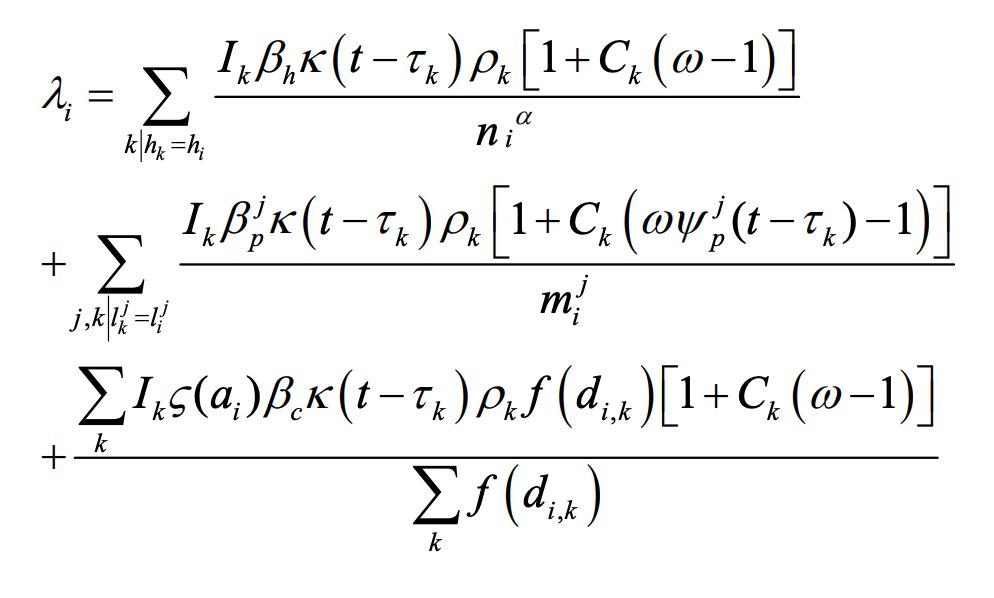
But the punchline is that there are separate transmission coefficients for household, place (schools and workplace classes), and community and some details associated with household or place size, individual infectiousness, and differences in infectiousness with severe cases, etc
They calibrate the model for 1/3 of transmission to occur at school/work, home, and in community. Community contact rates ς(a_i) depend on age. Severe cases given by C above occur 50% of the time and are more likely to be detected and isolated but are also more infectious.
They assume that symptomatic people are 50% more infectious than asymptomatic and individual infectiousness also varies probabilistically. In their scenarios, school closures increase transmission in the home 50% and in community by 25%.
Basically, there is substantial uncertainty, but the punchline is that social distancing, home isolation of cases, and school closure would have the largest impact, but you'd have to implement these policies for a long time. Doing this for 18 months seems untenable. So now what?
I hope we're going to learn from South Korea that a large workforce of people doing fever checks, massive testing, and contact tracing can help keep cases very low once society resumes. Korea will reopen schools soon and we'll see what happens.
If massive testing and contact tracing works, we will need to build a workforce to do this, perhaps as part of a stimulus package. To keep the economy going, what better way than to employ many people to do disease surveillance and check fevers at supermarkets, schools, etc.










