1/ 💭Thoughts of a trainee💭
“Should I call my [resident/fellow/attending]?”
“I don’t want to be a bother.”
“I don’t want them to think I’m dumb.”
Sound familiar?
I know these thoughts plagued me.
How can we prevent this?
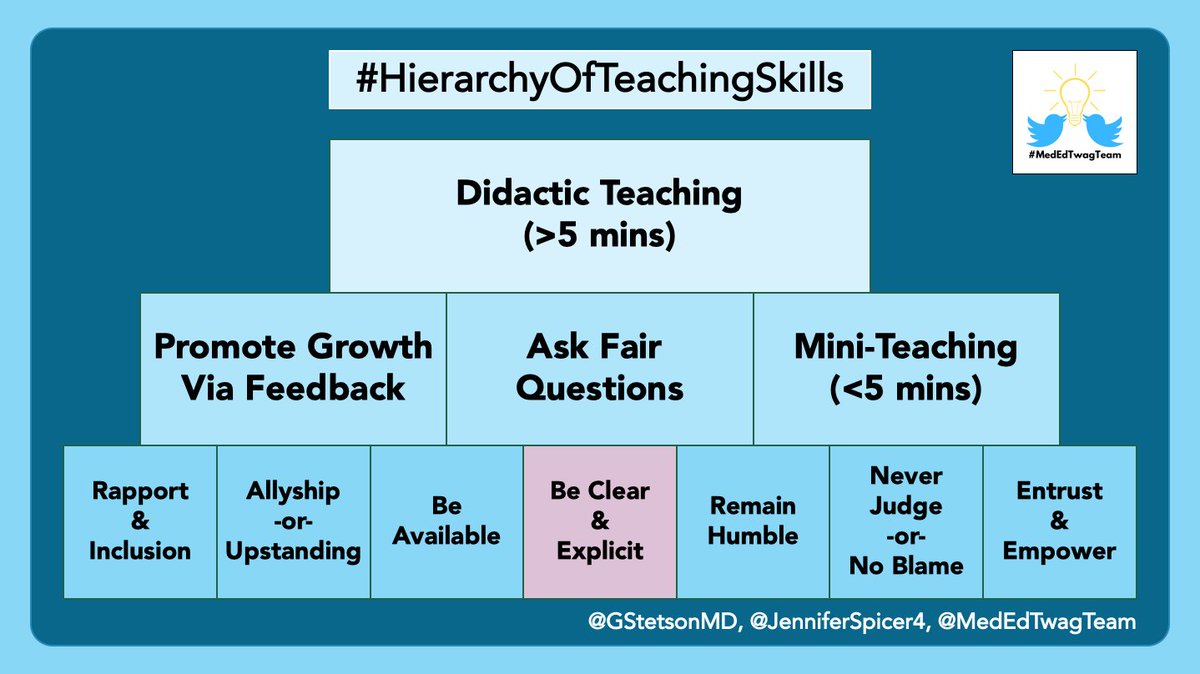
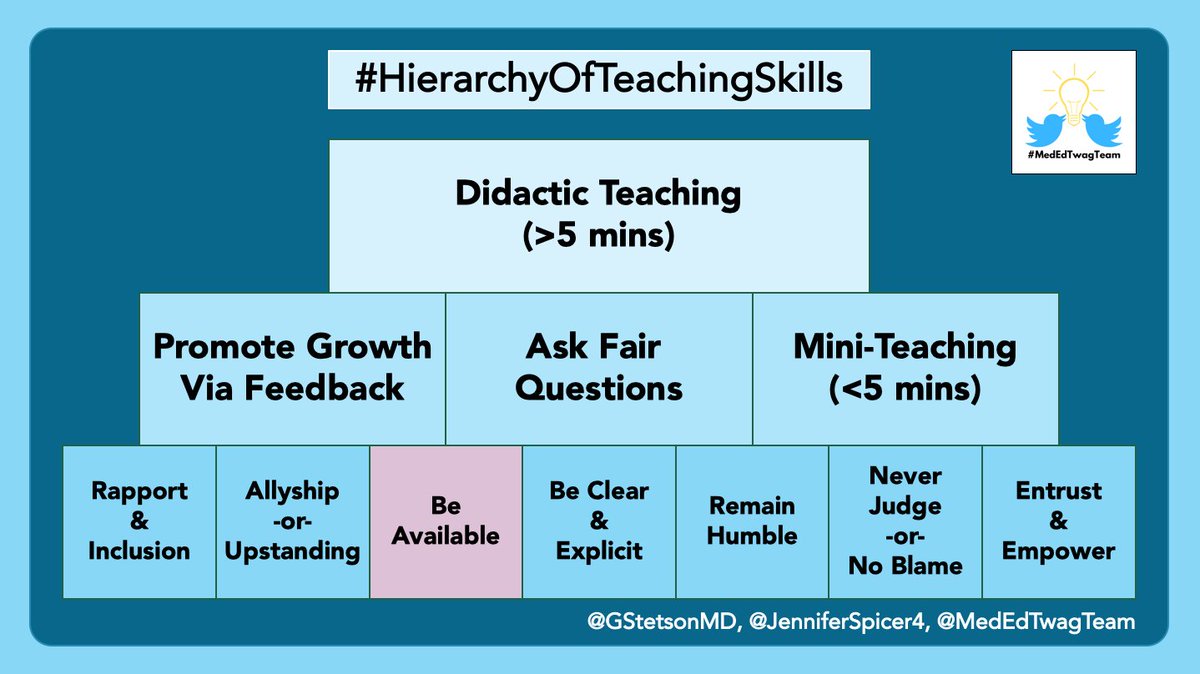
This week’s #ClinicalTeaching topic: Be Available
“Should I call my [resident/fellow/attending]?”
“I don’t want to be a bother.”
“I don’t want them to think I’m dumb.”
Sound familiar?
I know these thoughts plagued me.
How can we prevent this?
This week’s #ClinicalTeaching topic: Be Available
2/ To me, “Being Available” means ensuring that my team feels that I am their safety net
Nothing is beneath me.
I’m here to help.
WE, as a team, are responsible for our patients.
A failure of one, is a failure of all.
Yet, an accomplishment of one should be celebrated by all.
Nothing is beneath me.
I’m here to help.
WE, as a team, are responsible for our patients.
A failure of one, is a failure of all.
Yet, an accomplishment of one should be celebrated by all.
3/
In my mind, the concept of “Being Available” has two components:
1⃣Approachability (i.e. are people comfortable asking for help?)
2⃣Proximity (i.e. are you physically & mentally “there” for your team?)
In my mind, the concept of “Being Available” has two components:
1⃣Approachability (i.e. are people comfortable asking for help?)
2⃣Proximity (i.e. are you physically & mentally “there” for your team?)
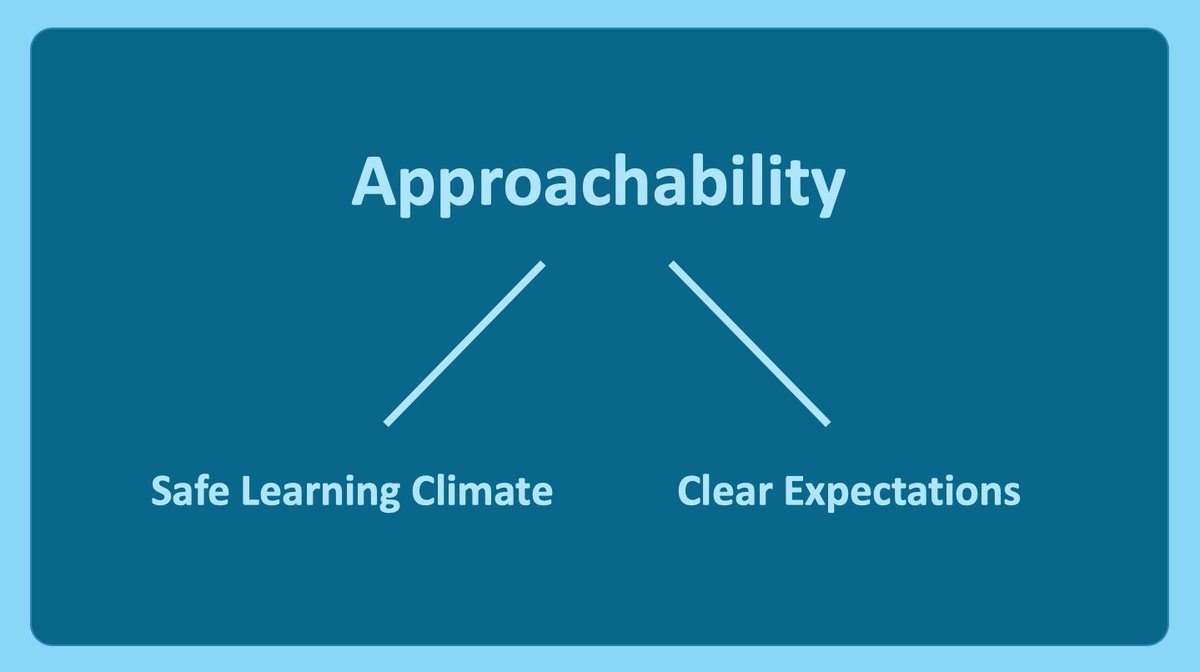
4/ Approachability has two inter-related aspects:
👉 Creating a safe learning climate
👉 Setting clear expectations
👉 Creating a safe learning climate
👉 Setting clear expectations
5/ A safe learning climate means that team members are comfortable being vulnerable.
Imposter syndrome is prevalent in medicine:
link.springer.com/article/10.100…
We should encourage team members to ask questions.
...And answer those questions.
Saying "look it up" is not always helpful
Imposter syndrome is prevalent in medicine:
link.springer.com/article/10.100…
We should encourage team members to ask questions.
...And answer those questions.
Saying "look it up" is not always helpful
6/ Setting clear expectations regarding availability is helpful
As a trainee, I found myself worrying about “bothering” people when I called.
As attendings/fellows/residents, we should set the expectation that needing help is normal & reiterate that people should call if needed
As a trainee, I found myself worrying about “bothering” people when I called.
As attendings/fellows/residents, we should set the expectation that needing help is normal & reiterate that people should call if needed
7/ Go beyond saying “call if needed” & be explicit.
I tell trainees they can contact me anytime when I’m awake (5:00 am – 9:00 pm), & ANYTIME for the following:
If a patient decompensates
If a patient tries to leave AMA
If a time-sensitive decision needs to be made
I tell trainees they can contact me anytime when I’m awake (5:00 am – 9:00 pm), & ANYTIME for the following:
If a patient decompensates
If a patient tries to leave AMA
If a time-sensitive decision needs to be made
8/ Now let’s talk about proximity.
When I say proximity, I mean both:
👉 Physical proximity (i.e. in the same room, hospital, etc)
👉 Mental proximity (i.e. not staring at your phone, thinking of something else, etc)
When I say proximity, I mean both:
👉 Physical proximity (i.e. in the same room, hospital, etc)
👉 Mental proximity (i.e. not staring at your phone, thinking of something else, etc)
9/ First, especially as an attending, try to be “mentally present” for your team by blocking off your schedule.
⭐️ Avoid scheduling research meetings, other educational obligations, etc
⭐️ Cancel as many non-essential recurring meetings as possible
⭐️ Avoid scheduling research meetings, other educational obligations, etc
⭐️ Cancel as many non-essential recurring meetings as possible

10/
Then, during rounds, pay attention.
✅ Use active learning techniques
✅ Use positive, open body language
✅ Avoid glancing at your phone
✅ Avoid looking at the patient's chart
And, if presentations are too long, then provide feedback instead of tuning out!
Then, during rounds, pay attention.
✅ Use active learning techniques
✅ Use positive, open body language
✅ Avoid glancing at your phone
✅ Avoid looking at the patient's chart
And, if presentations are too long, then provide feedback instead of tuning out!
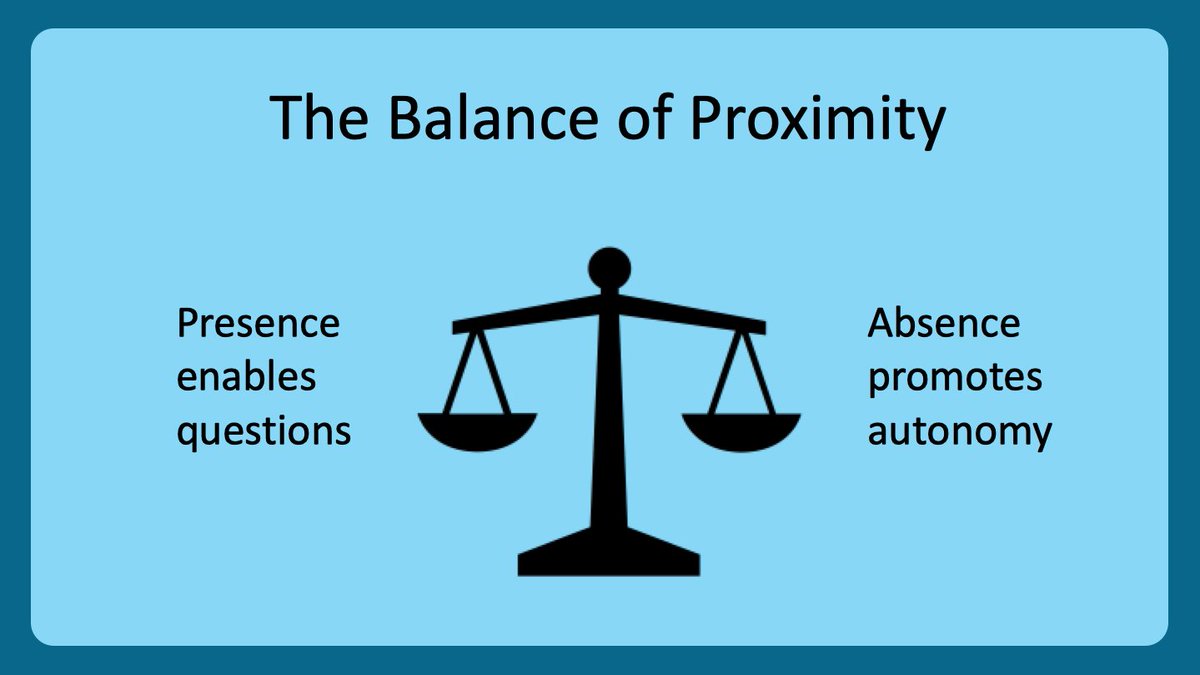
11/ Physical proximity lowers the barrier to ask questions, which has pros & cons.
Being present makes it easier for others to ask you questions.
This can be good.
But significant learning also occurs when learners are on their own (eg. nightfloat)
Appropriate balance is key
Being present makes it easier for others to ask you questions.
This can be good.
But significant learning also occurs when learners are on their own (eg. nightfloat)
Appropriate balance is key
12/ So what’s the ideal physical proximity?
It probably depends who you are on the team:
*⃣ Attending: stay during rounds, then let team do work
*⃣ Fellow: stay until residents done with notes
*⃣ Residents: stay until the team’s work is done
It probably depends who you are on the team:
*⃣ Attending: stay during rounds, then let team do work
*⃣ Fellow: stay until residents done with notes
*⃣ Residents: stay until the team’s work is done
13/ Staying until the work is done helps:
⭐️Fellows⭐️
Residents will write better consult notes b/c they are more likely to ask detail-oriented questions
⭐️Residents⭐️
Interns will appreciate you helping them with work; plus, you will know more about their workflow & efficiency
⭐️Fellows⭐️
Residents will write better consult notes b/c they are more likely to ask detail-oriented questions
⭐️Residents⭐️
Interns will appreciate you helping them with work; plus, you will know more about their workflow & efficiency
14/ And as an intern, being available to medical students is important & rewarding.
You have lots to teach.
And you can help the students shine on rounds.
Just set clear expectations with students to maximize learning & patient care
(more on this next week from @GStetsonMD!)
You have lots to teach.
And you can help the students shine on rounds.
Just set clear expectations with students to maximize learning & patient care
(more on this next week from @GStetsonMD!)
15/ So, in summary, be your team’s safety net using these concepts:
Approachability:
✅ Create a safe learning climate
✅ Set clear expectations regarding availability
Proximity:
✅ Be physically close (while allowing autonomy)
✅ Be mentally present to the team
Approachability:
✅ Create a safe learning climate
✅ Set clear expectations regarding availability
Proximity:
✅ Be physically close (while allowing autonomy)
✅ Be mentally present to the team
16/ And keep an eye out for @GStetsonMD’s thread next Tuesday on ”Be Clear & Explicit”
And check out the @MedEdTwagTeam if you want to see all of our threads in one place!
Thanks for joining, and we will see you next week!
And check out the @MedEdTwagTeam if you want to see all of our threads in one place!
Thanks for joining, and we will see you next week!