@hahn_rt 📝 #ASEchoJC
Can a single cycle length method can be used to calculate aortic EOA in aortic stenosis w nonsinus rhythms?
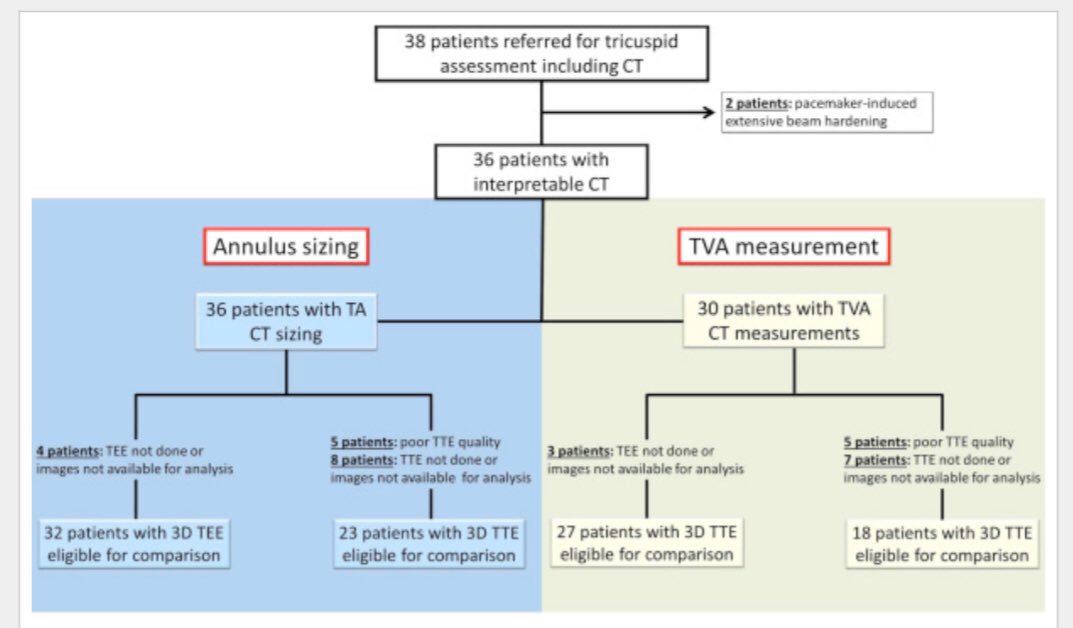
100 AS pts w R-R variability identified:55 w atrial fib AF & 45 w frequent atrial or ventricular premature contractions FE bit.ly/3or3ufk
Can a single cycle length method can be used to calculate aortic EOA in aortic stenosis w nonsinus rhythms?
100 AS pts w R-R variability identified:55 w atrial fib AF & 45 w frequent atrial or ventricular premature contractions FE bit.ly/3or3ufk


2/#ASEchoJC
LVOT TVI by PWD & AV VTI CWD measured over 5-10 consecutive beats in AF group & over 3-5 consecutive sinus beats in FE,EOA & DVI calculated as guidelines standard
In all patients, LVOT diameter was measured in midsystole, within 2-4 mm apical to annulus
LVOT TVI by PWD & AV VTI CWD measured over 5-10 consecutive beats in AF group & over 3-5 consecutive sinus beats in FE,EOA & DVI calculated as guidelines standard
In all patients, LVOT diameter was measured in midsystole, within 2-4 mm apical to annulus




3/#ASEchoJC Aortic EOA & DVI Calculated by Single Cycle Length Method
RR intervals matched
AF pts, a single VTIAV was measured & then matched to a VTILVOT of similar cycle length defined as R-R intervals w/in 10% of each other,EOA & DVI calculated for short & long R-R cycles
RR intervals matched
AF pts, a single VTIAV was measured & then matched to a VTILVOT of similar cycle length defined as R-R intervals w/in 10% of each other,EOA & DVI calculated for short & long R-R cycles


4/ In patients in FE group, only a long R-R cycle was measured: a VTIAV following a postectopic beat was measured & matched to a VTILVOT following a postectopic beat of similar cycle length. EOA and DVI were calculated from the postectopic beat #ASEchoJC

5/ Findings: #ASEchoJC
No significant differences in RR cycle lengths between VTI LVOT & VTI AV for standard & single cycle length methods long & short cycles in AFib or in FE pts cycle lengths for sinus beats or long postectopic cycles
No significant differences in RR cycle lengths between VTI LVOT & VTI AV for standard & single cycle length methods long & short cycles in AFib or in FE pts cycle lengths for sinus beats or long postectopic cycles

6/Findings: SV
AF pts,SV 63.5 ± 17.6 mL by standard method > than SV 55.1 ± 17.6 mL by single cycle length short R-R cycle & < than SV 72.8 ± 21.2 mL by single cycle length long RR cycle
FE SV 96.1 ±28.2 mL postectopic beat larger >SV 77.9 ± 23.2 mL from sinus rhythm #ASEchoJC
AF pts,SV 63.5 ± 17.6 mL by standard method > than SV 55.1 ± 17.6 mL by single cycle length short R-R cycle & < than SV 72.8 ± 21.2 mL by single cycle length long RR cycle
FE SV 96.1 ±28.2 mL postectopic beat larger >SV 77.9 ± 23.2 mL from sinus rhythm #ASEchoJC

7/#ASEchoJC
AFib:By single cycle length method, no difference in EOA with long R-R cycles but with short R-R cycles EOA DVI larger than standard approach
FE group, postectopic beat had larger EOA & DVI c/w standard approach
👍Correlation EOA by Standard🆚Single Cycle Length
AFib:By single cycle length method, no difference in EOA with long R-R cycles but with short R-R cycles EOA DVI larger than standard approach
FE group, postectopic beat had larger EOA & DVI c/w standard approach
👍Correlation EOA by Standard🆚Single Cycle Length

Will discuss Join us 8p
1. matching cycle lengths for VTILVOT & VTIAV high correlation w standard EOA
2. AF pts single long R-R cycle most accurate method for EOA for AS pts
3.FE postsystolic beat higher peak transaortic gradient, larger SV, larger EOA c/w sinus beats #ASEchoJC
1. matching cycle lengths for VTILVOT & VTIAV high correlation w standard EOA
2. AF pts single long R-R cycle most accurate method for EOA for AS pts
3.FE postsystolic beat higher peak transaortic gradient, larger SV, larger EOA c/w sinus beats #ASEchoJC

• • •
Missing some Tweet in this thread? You can try to
force a refresh