,
16 tweets,
9 min read
Read on Twitter
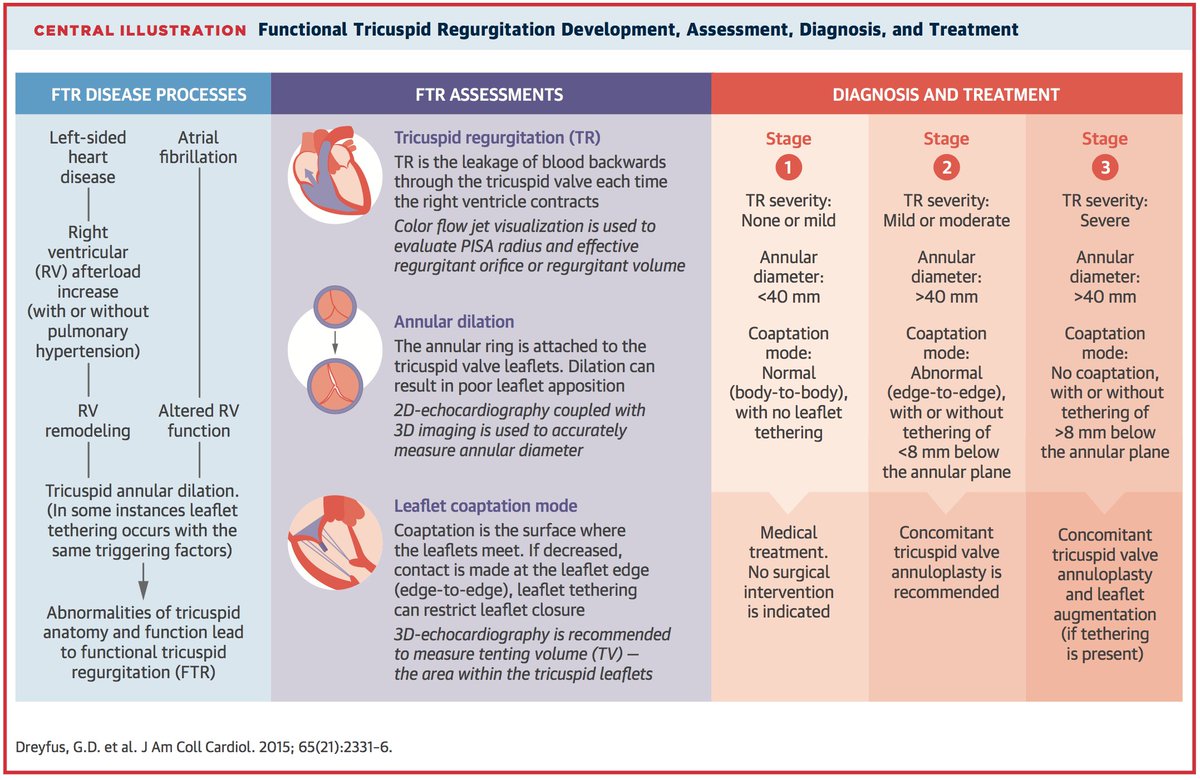
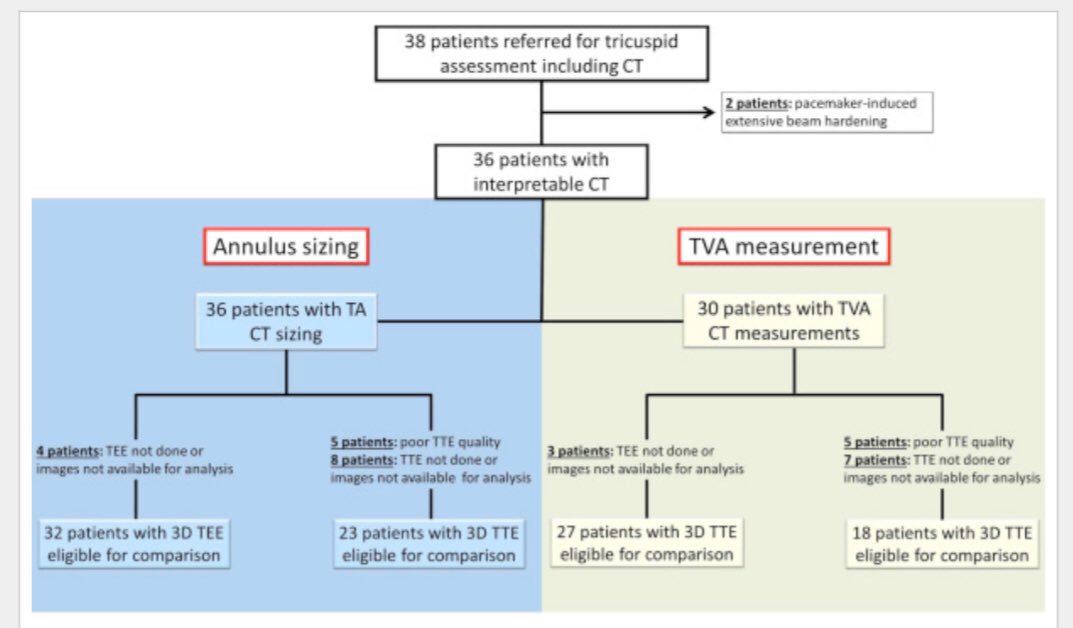
1/#Tweetorial 3D Echo(TTE/TEE) & CT methods Tricuspid annulus & valve assessment in severe TR #ASEechoJC Today 8 pm
bit.ly/2FFWk3I
pts with severe tricuspid regurgi, semiautomated indirect planimetry results in agreement b/w TEE & CT for Tricuspid annulus sizing & TVA
bit.ly/2FFWk3I
pts with severe tricuspid regurgi, semiautomated indirect planimetry results in agreement b/w TEE & CT for Tricuspid annulus sizing & TVA
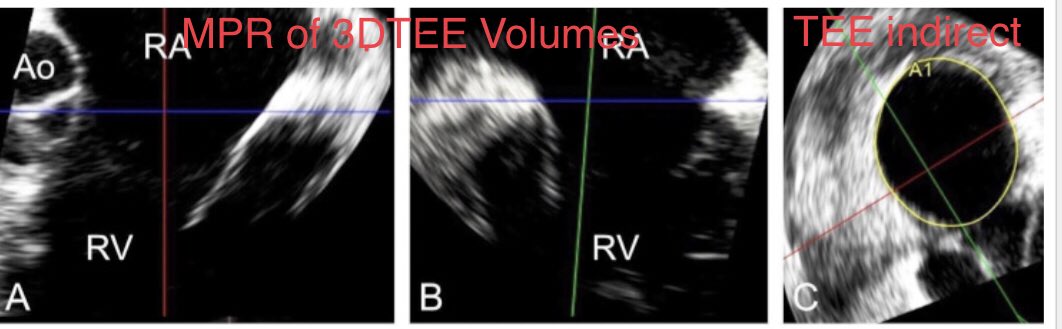
2/TEE_direct of the TA allows the most accurate measurement of diastolic stroke volume for the calculation of regurgitation severity compared with 3D vena contracta area.
This is first study to validate use of 3D TEE planimetered annular area to quantify the regurgitant volume
This is first study to validate use of 3D TEE planimetered annular area to quantify the regurgitant volume

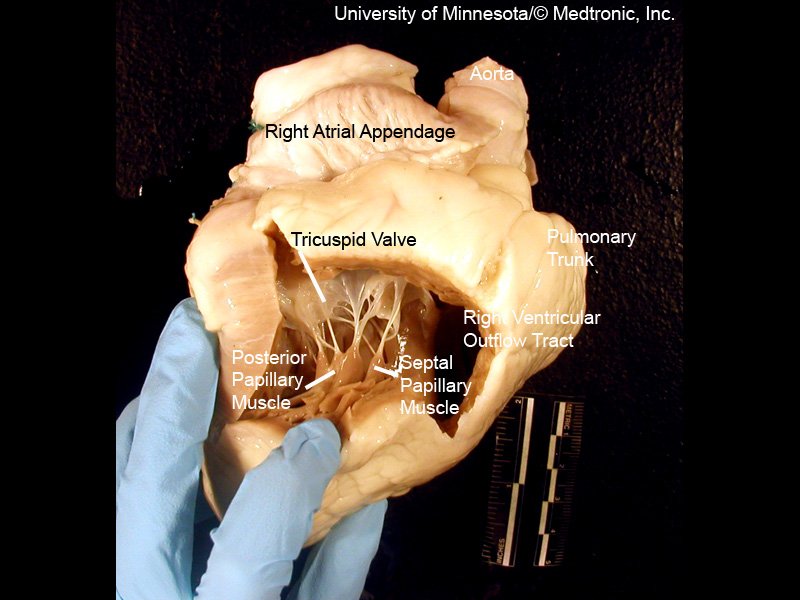
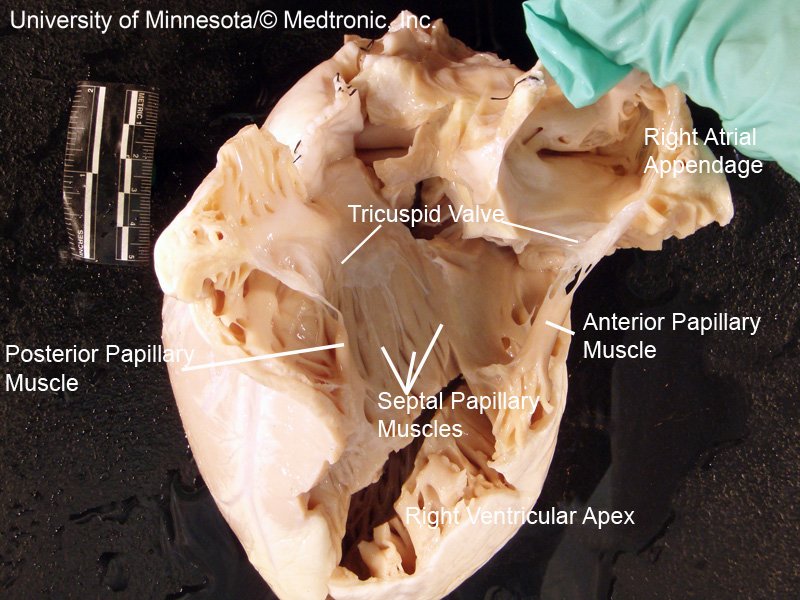
3/Imaging tricuspid valve (TV) is challenging & often requires nonstandard views because of variable anatomy, thin valve leaflets, shadowing/artifacts from the lungs, L sided valve prostheses/intracardiac leads, & the anterior position of the right ventricle inside of the chest
4/diastolic SV calculated by TA annular area by TEE & CT,
TA area x PWD VTI at annular plane. The stroke volume from LVOT/RVOT ( +/- AI/PI) was -from the diastolic SV to get RV
RV div by TR VTI (CWD) =EROA
This EROA compared to 3D vena contracta area (VCA) by 3D Doppler planime
TA area x PWD VTI at annular plane. The stroke volume from LVOT/RVOT ( +/- AI/PI) was -from the diastolic SV to get RV
RV div by TR VTI (CWD) =EROA
This EROA compared to 3D vena contracta area (VCA) by 3D Doppler planime



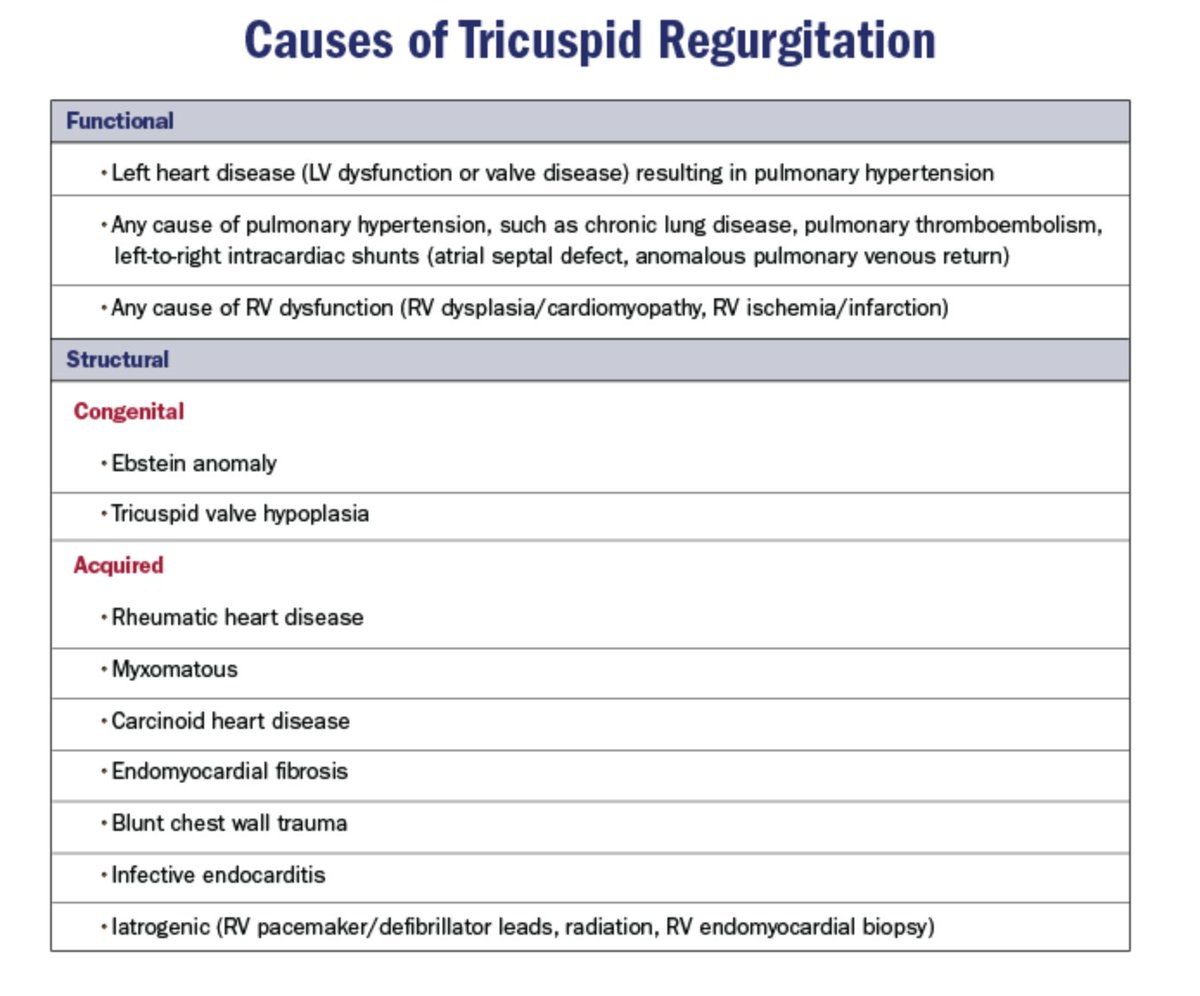
5/there was a significant correlation between 3D VCA & the size of the tricuspid annulus & emphasizes predominant role of annular dilatation in the development of functional TR;annular area may be considered as an indirect indicator of TR severity.


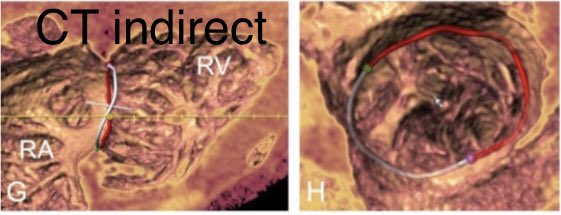
6/CT with quanitification software for both TA sizing & TVA measurement during diastole. Direct planimetry of the TVA appears to overestimate the semiautomated CT Tricuspid annulus dimensions
explained by several factors
explained by several factors


7/as the tricuspid annulus remodels in the setting of severe TR, the annular shelf protrudes (Figure 8A), & the transition between the shelf and the leaflet may not be clearly visible on the short axis (Figures 8B & 8D)

8/because of the nonplanar annulus, a short-axis view of the tricuspid annulus will be off the plane of the true annulus in two positions, typically within the atrium (Figure 8C), and thus overestimate the true area

9/TEE direct planimetry tends to underestimate semiautomated TEE TA dimensions related not only to the saddle shape of the annulus but also to the limited lateral resolution of echo affecting direct planimetry from a short-axis view more than the semiautomated measurements



10/that uses “long-axis” views (perpendicular to annular plane) to help locate the level of the annulus by identifying important anatomic landmarks (i.e., hinge point of the leaflets & adjacent structures) thus does not rely only on lateral resolution but also uses axial resoluti



11/In addition, seeing the motion of these structures in the long-axis views may improve recognition of artifacts such as side lobes.
Severe valve tethering frequently observed in advanced TR may contribute to the annular area underestimation by TEE direct planimetry because
Severe valve tethering frequently observed in advanced TR may contribute to the annular area underestimation by TEE direct planimetry because

12/accentuated leaflet curvature may translate into the apparition of a double contour on the short-axis plane as shown in Figure 7.
Misinterpretation of the inner line as the annular border will result in significant underestimation of the TA area.
Misinterpretation of the inner line as the annular border will result in significant underestimation of the TA area.

13/In patients with severe tethering or RV pacemaker lead semiautomated methods should be preferred with both CT & TEE imaging for optimal delineation of the annulus-leaflet hinge points. Severe beam-hardening artifact from pacemaker leads limit the feasibility of CT measurement

14/limitations to measurement of 3D color VCA, include limited lateral resolution, variability of the regurgitant orifice during the cardiac cycle, & risk for inappro- priate plane placement (in particular with regard to the complexity of the TR regurgitant orifice)
15/Implications for TR Grading
Patients with severe TR tend to present late in part because of PISA use for quantitation & thus underestimation of disease;extended grading scheme👇🏻
*However, best imaging method for quantifying the diastolic stroke volume has🚫yet been determined
Patients with severe TR tend to present late in part because of PISA use for quantitation & thus underestimation of disease;extended grading scheme👇🏻
*However, best imaging method for quantifying the diastolic stroke volume has🚫yet been determined
16/perimeter appears more reliable between techniques-varies less during the cardiac cycle than area & often measurements made not at the exact same time
For this reason, future sizing guidelines as well as result assessment after annuloplasty may rather focus on perimeter
For this reason, future sizing guidelines as well as result assessment after annuloplasty may rather focus on perimeter