THREAD: Some thoughts on trust and transparency when leading people/teams, related to recent data & report re: schools & #COVID19 in ON
For a great thread check out @DocDominik's take.
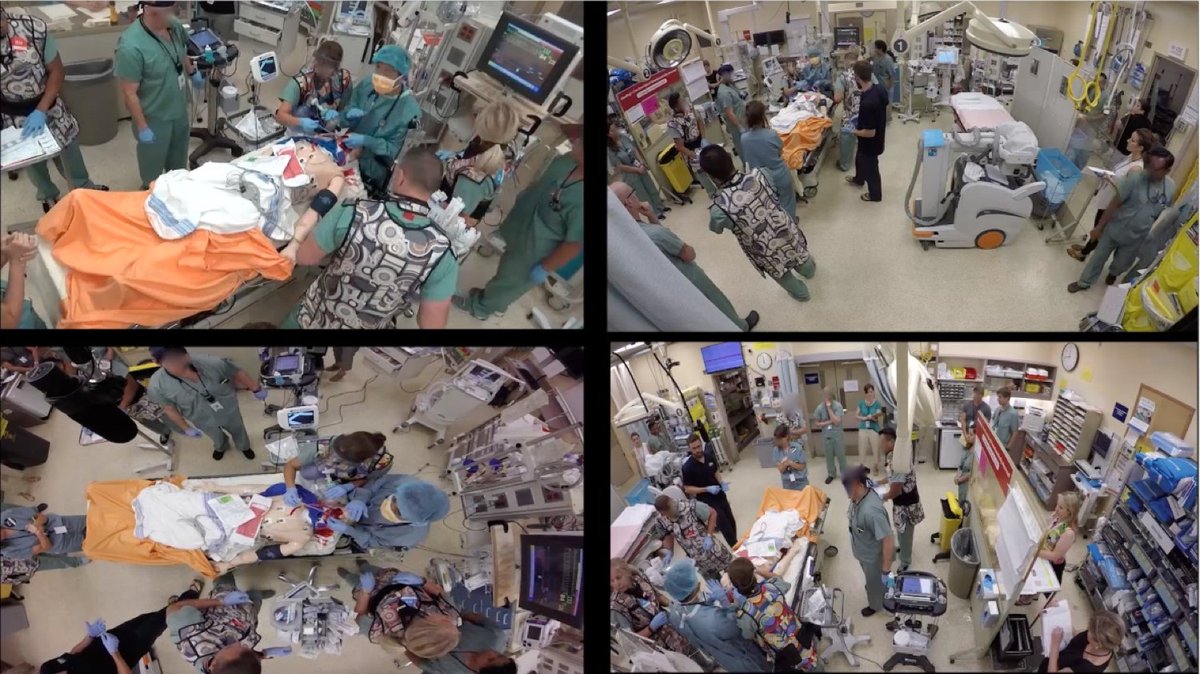
My take relates to crisis management & influencing behavior
1/
For a great thread check out @DocDominik's take.
https://twitter.com/DocDominik/status/1352320629106728961
My take relates to crisis management & influencing behavior
1/

I’m not qualified to comment on whether school closure should continue or not. (personally, as a parent of a 4yr old...please re-open! but not the point here)
Some considerations
2/
Some considerations
2/
1. Transparency: when reports are leaked, there’s high prob for misunderstanding. Transparency in the long run is often the preferred approach (except maybe national security) but it is very true that lack of transparency fosters further mistrust.
bit.ly/397ihX8
3/
bit.ly/397ihX8
3/
The gov’t decided to keep schools closed…that should be paired with data that informed that decision (e.g. school reports)
4/
4/
2. Hind sight bias: This point is for us as the public. We’ll inevitably 2nd guess gov’t officials but lets remember they made a decision with the information they had then, not what we have now. This drastically influences how we evaluate decisions.
5/
5/

Also, decisions should be thought of probabilistically. E.g. "we think with 90% certainty, closing schools is the right move." That doesn't mean it's right...in 10% of futures, its wrong. Unfortunately this isn't an intuitive method for humans...but the media can help here.
6/
6/
3. Quick first step: we teach this in crisis management, take action but favor safety. Tbh, that’s what the gov’t did. They made the decision, extend school closures. I support that, not because I want them closed but because they didn’t have control over the situation.
7/
7/

If you don't have control...select the safest option ("fail safely"...temporarily), buy yourself time, evalulate options then decide on whether to pivot. But let your "team" or "the public" know exactly what you're doing...there's that term again...transparency.
8/
8/
This buys time. But time must be used wisely to build a plan to reduce risks in schools (has this happened?). Also add the “why”…which hasn’t been well articulated. We hear schools are both safe & unsafe. This is confusing. Rather abandon this talk risk as a spectrum
9/
9/
4. Data driven decisions –we heard from CMOH that we need <150 ICU patients and <1000 cases/d before lockdown opens. This needs to be more closely linked with why these numbers are chosen.
Many have discussed NB of data incl @ASPphysician @BogochIsaac @jkwan_md @IrfanDhalla
10/
Many have discussed NB of data incl @ASPphysician @BogochIsaac @jkwan_md @IrfanDhalla
10/
5. Show the public what you’ve done during this lockdown to invest in re-opening. We’ve all locked down, now time for the relationship to be reciprocal
11/
11/

6. More transparency: Feb 10th…many of us literally can't wait until this day...but there's a chance schools still don't re-open...which I accept if this is based on best available information & risks to our society...
12/
12/
…but we can provide several models that would/wouldn’t allow schools to open. E.g. “Feb 10, we plan to open schools if we can achieve X & Y. We also know theres some unpredictable factors that might force us to continue closures...
13/
13/
...but we believe with high degree of certainty they’ll re-open, so let’s make it happen...and here's what we need from each of you”
14/
14/
7. If you want people to buy into a plan, you only get blind trust for so long before they question goals/objectives and need the "WHY". And probably needs to be more than just "because our system is overwhelmed".
15/
15/
While that is true, recognize the message may be losing its power/influence.
Summary:
- Help us understand the WHY, as intelligent individuals.
- Favour transparency when in doubt
- Be explicit with metrics (but call out ahead of time...we may get it wrong)..honestly.
END
Summary:
- Help us understand the WHY, as intelligent individuals.
- Favour transparency when in doubt
- Be explicit with metrics (but call out ahead of time...we may get it wrong)..honestly.
END
• • •
Missing some Tweet in this thread? You can try to
force a refresh