1/8 Let's review assessment of hypovolemia based on physical exam. (yes, I know #POCUS is SO valuable in making this assessment)
Which physical exam finding is most useful to detect hypovolemia in adults?
#MedTwitter #FOAMed #MedEd #MedStudentTwitter
Which physical exam finding is most useful to detect hypovolemia in adults?
#MedTwitter #FOAMed #MedEd #MedStudentTwitter
2/8 According to a great review by Dr. McGee in JAMA Rational Clinical Exam "Is This Patient Hypovolemic" the answer is... sunken eyes!
jamanetwork.com/journals/jama/…
jamanetwork.com/journals/jama/…
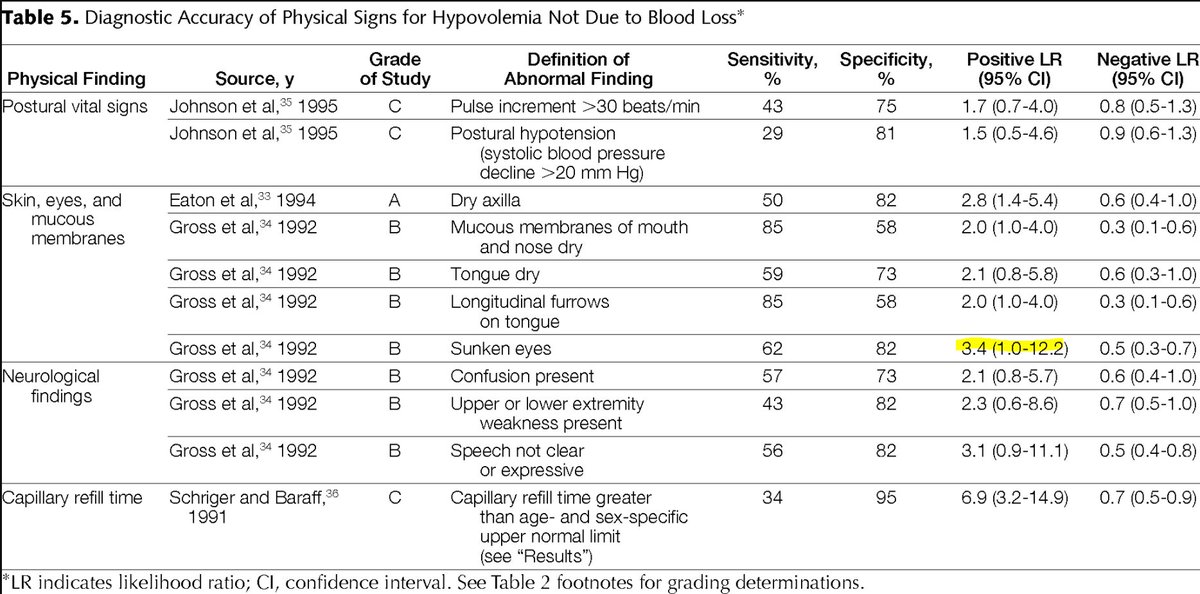
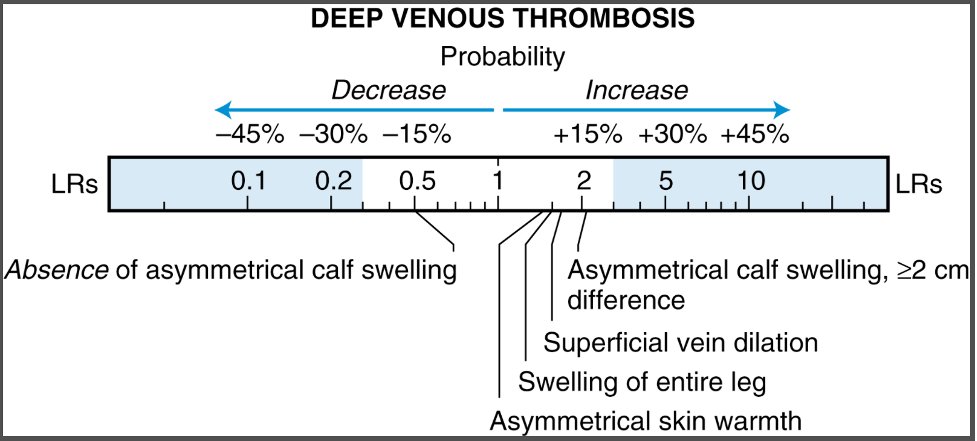
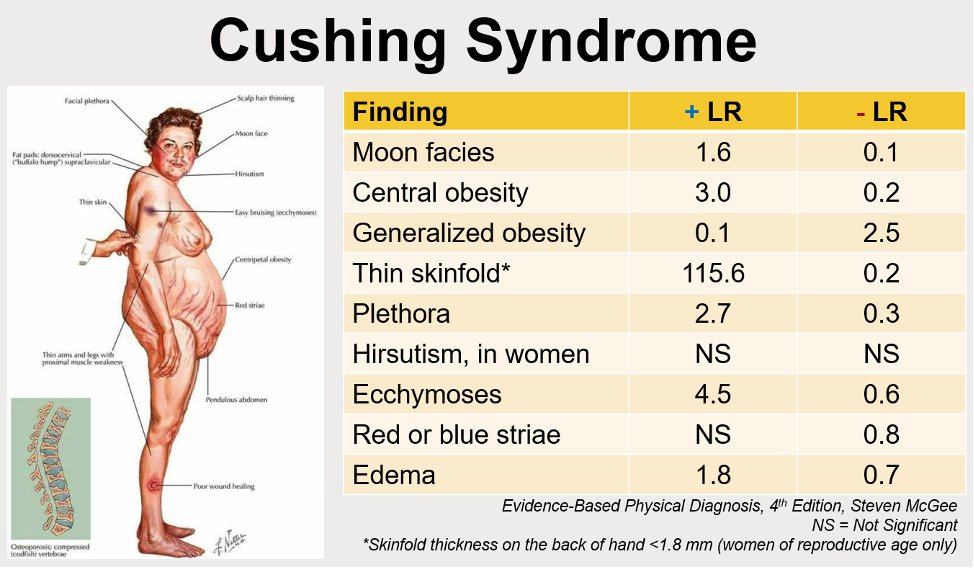
3/8 For a way to clinically interpret the LRs, let's turn our attention to Dr. McGee's book "Evidence-Based Physical Diagnosis." Although sunken eyes has the highest LR, notice how small the difference in increase in probability there is with each exam finding.

4/8 To understand why this is, it can be helpful to look at the Fagan nomogram used to calculate post-test probability based on LR.
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…

5/8 So how do we use this thing? It requires you to have a sense of the pre-test probability (which you mark on the left side) and draw a line through the LR. Here's a great example that shows you how 2 different LRs influence post-test probability.
researchgate.net/publication/29…
researchgate.net/publication/29…

6/8 This (hopefully) helps visualize why you need quite a high LR or (rather low LR) to really influence your suspicion for something.
Remember that you cannot add the LRs of two findings and run it through the nomogram.
Remember that you cannot add the LRs of two findings and run it through the nomogram.
7/8 Last bit of info - if you decide to assess for skin turgor, you should do this in the subclavicular area, as elastin plays a large role in skin turgor in the extremities!
8/8 In summary:
⭐️Sunken eyes has the highest +LR for hypovolemia
⭐️Fagan nomograms show us that the LR needs to be really high or low to significantly change probability
⭐️Assess skin turgor in subclavicular area
⭐️Sunken eyes has the highest +LR for hypovolemia
⭐️Fagan nomograms show us that the LR needs to be really high or low to significantly change probability
⭐️Assess skin turgor in subclavicular area
• • •
Missing some Tweet in this thread? You can try to
force a refresh