Most of our misunderstandings come from semantics, using absolute binaries, without subtleties, for complex problem. Saying, e.g., just vaccines 'protect', with no additional explanations, suggests 100%, which is as unscientific as anti-vaxxer saying they don't work at all.
1/
1/
Those kind of positions are confrontational & destroy trust. When someone only says 'protect', I ask yes but HOW MUCH, AGAINST WHAT & HOW LONG? When someone says 'see, they don't work', I say they DO this much, against this & this long. I think that's how you build trust.
2/
2/
Hopefully, data will soon clarify current confusions, as there are more & more fantastic studies.
I would say, correct me if I'm wrong, that Abs are still our best correlate for protection. There are likely better ones, but we can't yet qualify or quantify them.
3/
I would say, correct me if I'm wrong, that Abs are still our best correlate for protection. There are likely better ones, but we can't yet qualify or quantify them.
3/
Based only on that, I still say the more Abs, the better the vaccine. But Abs obviously wane as they are supposed to; after 6 months, drop-off is significant enough to open a window of possibility for reinfection or breakthrough. Thus, boosters are necessary if NPIs abolished.
4/
4/
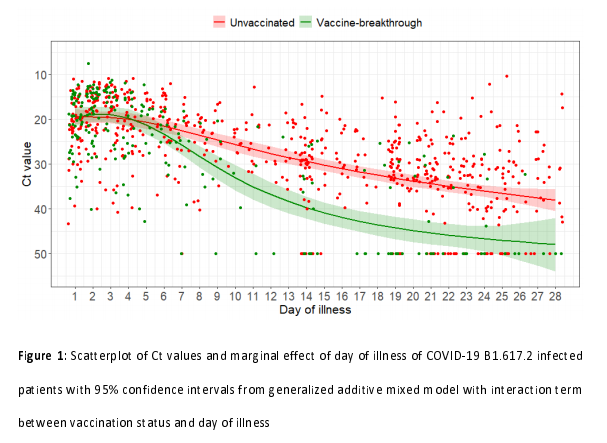
On the other side, #SARSCoV2 variants improved transmission, binding, replication and/or Abs evasion. It resulted in #Delta having a 1000 times higher viral load than the original. VOCs transmission & binding are also better at lower than higher temperature (humidity unknown).
5/
5/
Next, studies proved that for clearing upper airways we need higher Abs levels than for lower airways.
Also, kids are better at clearing the virus than adults thanks to greater & fresher innate immune memory in nasal mucosa (adaptive memory vs. #SARS2 is still under debate).
6/
Also, kids are better at clearing the virus than adults thanks to greater & fresher innate immune memory in nasal mucosa (adaptive memory vs. #SARS2 is still under debate).
6/
Why is then difficult to accept that if our diminishing protective army is confronted in the nose with increased numbers of the now disguised enemy, it might lead to reinfection or breakthrough?
If the fight continues, with time #SARS2 might even break to lower airways again.
7/
If the fight continues, with time #SARS2 might even break to lower airways again.
7/
So, when someone asks me, I give long answers. Vaccines certainly help & are absolutely needed as they are our best weapon. They offer some, but when excessively confronted with #Delta variant not much protection vs. infection, and just a little more vs. symptomatic #COVID.
8/
8/
If vaccinated get infected (test positive with or without symptoms), they most likely have less but more than enough viral load to transmit the virus to other vaccinated or not. Thus, they still need to carry masks indoors to protect themselves & limit the spread to others.
9/
9/
Repeated infections may boost immunity but are undesirable because each can do harm. For example, it seems vaccines can't protect against anosmia, which is a pathway to the brain. Also, 19% of breakthrough infections reported #LongCovid symptoms.
10/
10/
Vaccines offer much better, often life-saving protection vs. hospitalizations, severe #COVID & death. But, as Abs wane, it's unknown if & how long that will last. Thus, boosters are needed starting with the oldest & most frail again; until we find a longer-lasting solution.
11/
11/
• • •
Missing some Tweet in this thread? You can try to
force a refresh