
#LongCOVID
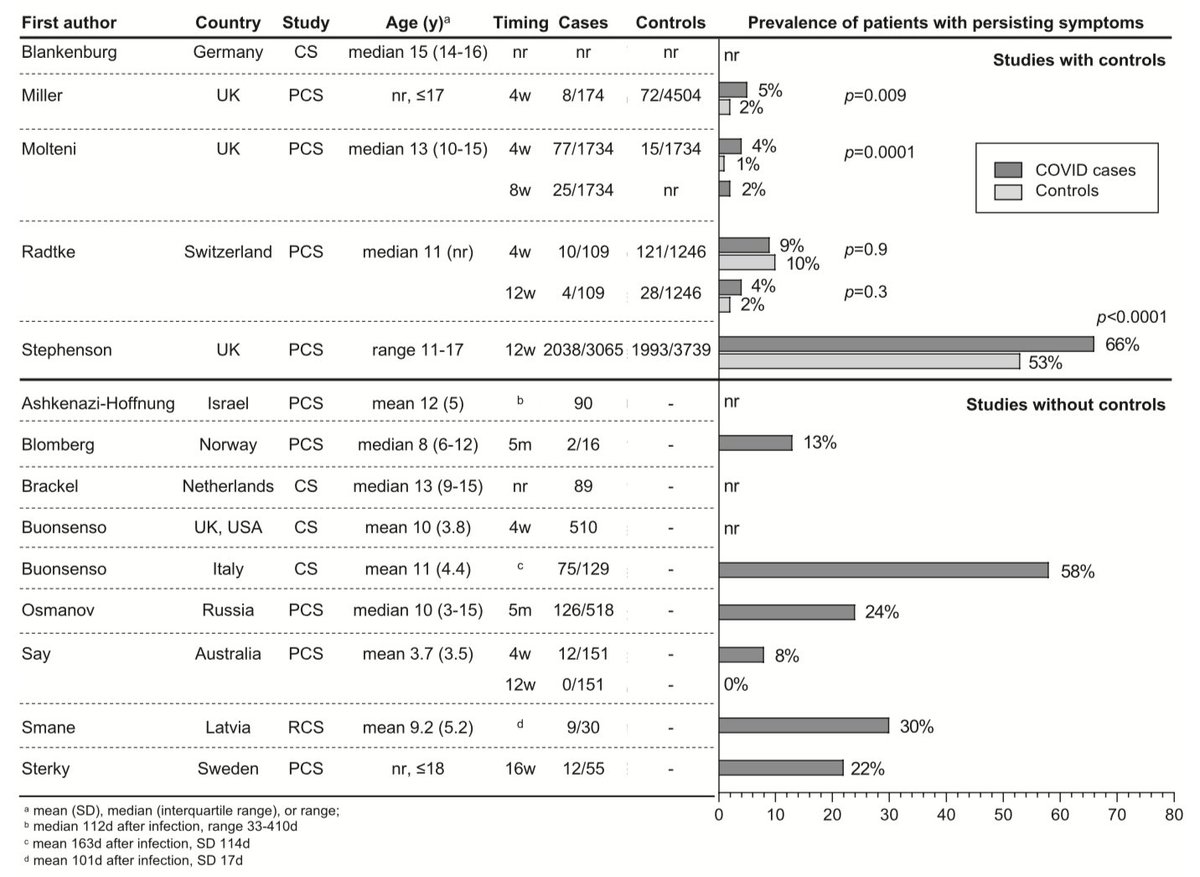
We reviewed 14 studies of persisting symptoms following #COVID19 in #children & #adolescents
Most had major limitations and should be interpreted with caution.
True risk is likely to be nearer 1 in 100 than often quoted 1 in 7.
#medpeds #IDTwitter
(Long) 🧵1/n
We reviewed 14 studies of persisting symptoms following #COVID19 in #children & #adolescents
Most had major limitations and should be interpreted with caution.
True risk is likely to be nearer 1 in 100 than often quoted 1 in 7.
#medpeds #IDTwitter
(Long) 🧵1/n
@Dr_Petzi @PittetLaure @MCRI_for_kids @RCHMelbourne @UniMelbMDHS @ASIDANZ @ESPIDsociety @ESPR_EBN @WSPID @PIDSociety @DFTBubbles @PIDJournal
#medpeds #IDTwitter #tweetiatrician #paediatrics #pediatrics #PaedsID #PedsID #PedID #PID
#medpeds #IDTwitter #tweetiatrician #paediatrics #pediatrics #PaedsID #PedsID #PedID #PID
The 14 studies involved 19,426 children & adolescents.
Common persistent symptoms reported 4-12 weeks after acute #COVID19 were:
•headache
•fatigue
•sleep disturbance
•concentration difficulties
•abdominal pain.
Symptoms rarely lasted more than 12 weeks.
Common persistent symptoms reported 4-12 weeks after acute #COVID19 were:
•headache
•fatigue
•sleep disturbance
•concentration difficulties
•abdominal pain.
Symptoms rarely lasted more than 12 weeks.
Long-term #SARSCoV2 infection-associated symptoms are difficult to distinguish from pandemic-associated symptoms.
Persistent symptoms were just as common in children & adolescents WITHOUT evidence of #SARSCoV2 infection in 2 of the 5 studies which included controls.
Persistent symptoms were just as common in children & adolescents WITHOUT evidence of #SARSCoV2 infection in 2 of the 5 studies which included controls.
Major limitation 1:
No clear case definition of #LongCOVID
• Studies use variable inclusion criteria & f/u times
• Some include self-reported #SARSCoV2 infection without lab confirmation
• Most rely on self/parent-reported symptoms from surveys w/o clinical assessment.
No clear case definition of #LongCOVID
• Studies use variable inclusion criteria & f/u times
• Some include self-reported #SARSCoV2 infection without lab confirmation
• Most rely on self/parent-reported symptoms from surveys w/o clinical assessment.
#LongCOVID encompasses many conditions:
• Complications such as pulm/myocardial dysfunction
• Mental health probs, post ICU syndr, PTSD
• Postviral chronic fatigue syndr/ME with nonspecific symptoms highly prevalent in population (e.g. sleep disturbance, conc difficulties).
• Complications such as pulm/myocardial dysfunction
• Mental health probs, post ICU syndr, PTSD
• Postviral chronic fatigue syndr/ME with nonspecific symptoms highly prevalent in population (e.g. sleep disturbance, conc difficulties).
Major limitation 2:
Just 5 studies had a control group NOT infected with #SARSCoV2 to enable differentiation between symptoms due to #COVID19 & those from effects of pandemic: lockdowns, school closures, social isolation, loss of sports/other activities, sick family/friends.
Just 5 studies had a control group NOT infected with #SARSCoV2 to enable differentiation between symptoms due to #COVID19 & those from effects of pandemic: lockdowns, school closures, social isolation, loss of sports/other activities, sick family/friends.
Major limitation 3:
Non-responder bias. Many studies have a low response rate (13% in CLoCk Study) that can lead to selection bias (those with persisting symptoms more likely to respond).
This can result in a substantial overestimate of the prevalence of #LongCOVID.
Non-responder bias. Many studies have a low response rate (13% in CLoCk Study) that can lead to selection bias (those with persisting symptoms more likely to respond).
This can result in a substantial overestimate of the prevalence of #LongCOVID.
Additional limitations:
• As those with mild symptoms might not seek testing, selection & misclassification bias also lead to an overestimate.
• Studies include a wide range of age groups: incidence & characteristics of #LongCOVID likely differ between adolescents & children.
• As those with mild symptoms might not seek testing, selection & misclassification bias also lead to an overestimate.
• Studies include a wide range of age groups: incidence & characteristics of #LongCOVID likely differ between adolescents & children.
An accurate determination of #LongCOVID risk in children & adolescents is crucial in weighing up the risks & benefits of vaccinating this age grp.
New studies should incl rigorous control grps of children with other infections & those admitted to hosp or ICU for other reasons.
New studies should incl rigorous control grps of children with other infections & those admitted to hosp or ICU for other reasons.
Key question for new #LongCOVID studies:
• What is age-specific risk?
• Is risk different with #DeltaVariant?
• Is risk related to severity of acute COVID?
• Can it follow asymptomatic infection?
• Does vaccination prevent it?
• Underlying immunol mechanisms?
• Treatment?
• What is age-specific risk?
• Is risk different with #DeltaVariant?
• Is risk related to severity of acute COVID?
• Can it follow asymptomatic infection?
• Does vaccination prevent it?
• Underlying immunol mechanisms?
• Treatment?
This fits with the latest ONS data that also suggests the risk of #LongCOVID in children & adolescents is extremely low (0% to 1.7%).
https://twitter.com/apsmunro/status/1438461046956646405
Importantly, even if only a very low % of children & adolescents have #LongCOVID, and regardless of whether their symptoms result from #SARSCoV2 infection or the indirect effects of the pandemic, we need to learn the best way to support them and help them get better.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


