1/ You're on the inpatient service,
and you want to teach...
but HOW are you supposed to FIND TIME ⏲️while also
✅ caring for patients
✅ writing notes
✅ completing other administrative work
Not to mention managing your personal life!
This week: tips on teaching BEFORE rounds
and you want to teach...
but HOW are you supposed to FIND TIME ⏲️while also
✅ caring for patients
✅ writing notes
✅ completing other administrative work
Not to mention managing your personal life!
This week: tips on teaching BEFORE rounds
2/ This week, I will share practical tips on how to integrate teaching into your daily routine BEFORE rounds.
It's another #TweetorialTuesday from the @MedEdTwagTeam for our #MedTwitter & #MedEd friends!
It's another #TweetorialTuesday from the @MedEdTwagTeam for our #MedTwitter & #MedEd friends!

When do you typically teach?
4/ As mentioned previously, I like to schedule teaching BEFORE rounds.
I do this because it:
*⃣ shows I PRIORITIZE teaching
*⃣ ensures we have TIME for teaching
*⃣ allows me to teach when learners are FRESH
Plus, it sets the tone for rounds as a time for teaching & learning.
I do this because it:
*⃣ shows I PRIORITIZE teaching
*⃣ ensures we have TIME for teaching
*⃣ allows me to teach when learners are FRESH
Plus, it sets the tone for rounds as a time for teaching & learning.
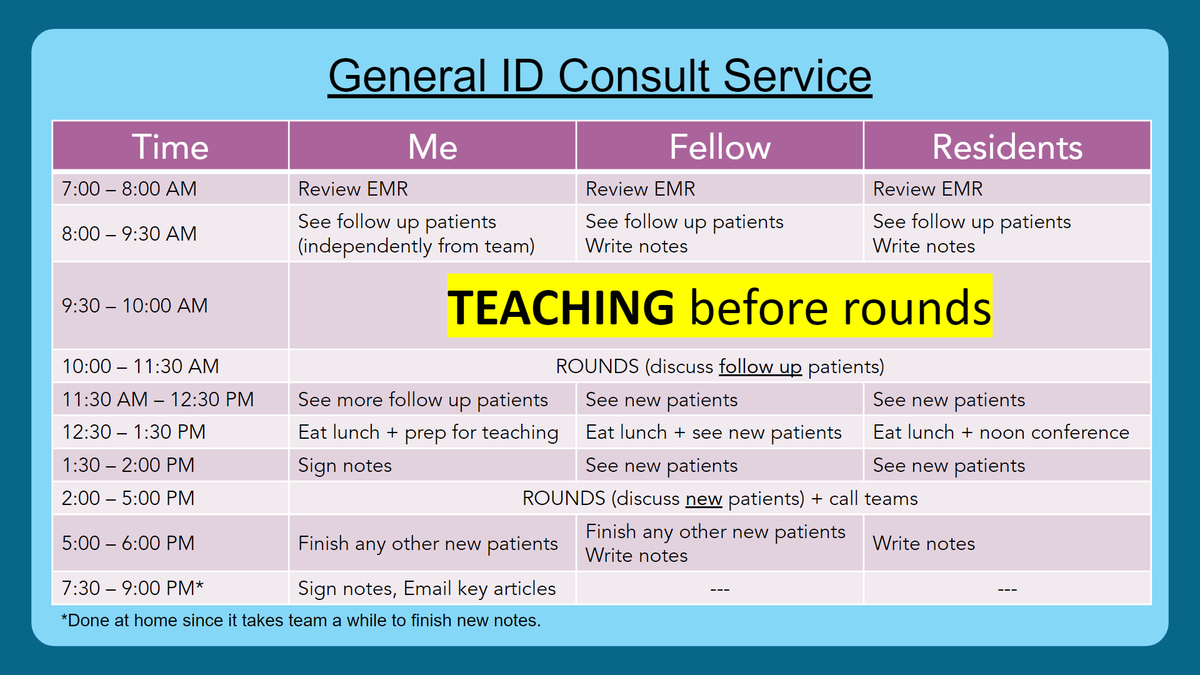
5/ When teaching before rounds, it's critical to pay attention to⏰
Keep it short or learners start worrying about how teaching is impacting their workflow.
Primary teams tend to have busier mornings than consult teams, so 5-10 minutes of teaching before rounds works best.
Keep it short or learners start worrying about how teaching is impacting their workflow.
Primary teams tend to have busier mornings than consult teams, so 5-10 minutes of teaching before rounds works best.
6/ There are many strategies that can be used for short, focused teaching sessions.
Here are 3 strategies that we have used/seen that are effective teaching methods.
(Alternatively, you can use the pre-round teaching time to get to know your team members!)
Here are 3 strategies that we have used/seen that are effective teaching methods.
(Alternatively, you can use the pre-round teaching time to get to know your team members!)

7/ Here are examples of peer teaching.
If you create a central repository to store the teaching points & learning resources, learners can reference it in the future!
Example: @ricapitt creates a Google slideshow & has learners add a slide w/ their teaching point each day.
If you create a central repository to store the teaching points & learning resources, learners can reference it in the future!
Example: @ricapitt creates a Google slideshow & has learners add a slide w/ their teaching point each day.

8/ Peer teaching benefits everyone.
1. Teaching is a powerful way to learn a concept better.
2. Peers' cognitive congruence with each other results in content being taught at the appropriate level.
3. It takes pressure off the attending.
Read more here:
tandfonline.com/doi/abs/10.108…
1. Teaching is a powerful way to learn a concept better.
2. Peers' cognitive congruence with each other results in content being taught at the appropriate level.
3. It takes pressure off the attending.
Read more here:
tandfonline.com/doi/abs/10.108…
9/ Retrieval practice refers to the process of having learners "retrieve" information from inside their head, usually by answering questions.
This is a great way to teach, and it requires very little prep from the teacher.
Here is how I use it for inpatient teaching.
This is a great way to teach, and it requires very little prep from the teacher.
Here is how I use it for inpatient teaching.

10/ If the concept of retrieval practice is new for you, use one of these excellent resources that summarize how to use it effectively:
An infographic:
learningscientists.org/retrieval-prac…
A video:
A website:
retrievalpractice.org
An infographic:
learningscientists.org/retrieval-prac…
A video:
A website:
retrievalpractice.org
11/ Bite-sized teaching sessions allow you to teach content in a short amount of time.
The key is to limit what is taught in a single session; however, the same topic can be covered over multiple sessions allowing more comprehensive coverage of a single topic, if desired.
The key is to limit what is taught in a single session; however, the same topic can be covered over multiple sessions allowing more comprehensive coverage of a single topic, if desired.

12/ Developing chalk talks will be covered in a future tweetorial.
For now, you can adapt others' chalk talks for your teaching. Examples:
*⃣@teachIM_org, teachim.org
*⃣@CPSolvers, clinicalproblemsolving.com
More about bite-sized teaching: bmcmededuc.biomedcentral.com/articles/10.11…
For now, you can adapt others' chalk talks for your teaching. Examples:
*⃣@teachIM_org, teachim.org
*⃣@CPSolvers, clinicalproblemsolving.com
More about bite-sized teaching: bmcmededuc.biomedcentral.com/articles/10.11…
13/ So, in summary, try to incorporate short 5-10 minute teaching sessions before rounds using:
*⃣ peer teaching
*⃣ retrieval practice
*⃣ bite-sized teaching sessions
Doing it at the beginning of rounds ensures that it happens, but make sure that you don't lose track of time!
*⃣ peer teaching
*⃣ retrieval practice
*⃣ bite-sized teaching sessions
Doing it at the beginning of rounds ensures that it happens, but make sure that you don't lose track of time!

14/ Are there other ways that you incorporate teaching before rounds? If so, please share!
Next week, stay tuned for @GStetsonMD who will discuss using questions for "priming".
See you then #MedTwitter #MedEd!
Next week, stay tuned for @GStetsonMD who will discuss using questions for "priming".
See you then #MedTwitter #MedEd!

• • •
Missing some Tweet in this thread? You can try to
force a refresh