Should #children be vaccinated against #COVID19?
Our review outlines the points to consider in weighing up whether all healthy children under 12y should be vaccinated against COVID-19.
bit.ly/2ZYyPi0
#medpeds #IDTwitter #PaedsID #tweetiatrician #paediatrics
🧵1/n
Our review outlines the points to consider in weighing up whether all healthy children under 12y should be vaccinated against COVID-19.
bit.ly/2ZYyPi0
#medpeds #IDTwitter #PaedsID #tweetiatrician #paediatrics
🧵1/n

As specialists in paediatric #InfectiousDiseases and #Vaccinology, we recognise enormous benefits of and strongly support child vaccination programmes
@Dr_Petzi @PittetLaure @adamhfinn @ajpollard1 @nigeltwitt
@unifr @unige_en @BristolUni @OxfordVacGroup @MCRI_for_kids @UniMelb
@Dr_Petzi @PittetLaure @adamhfinn @ajpollard1 @nigeltwitt
@unifr @unige_en @BristolUni @OxfordVacGroup @MCRI_for_kids @UniMelb
Our review highlights that the balance of risks and benefits of COVID-19 vaccination in children is more complex than in adults as the relative harms from vaccination and disease are less well established in this age group.
@ASIDANZ @ESPIDsociety @WSPID @PIDSociety @DFTBubbles
@ASIDANZ @ESPIDsociety @WSPID @PIDSociety @DFTBubbles
“… we do not argue for or against vaccinating children against COVID-19 but rather outline the points to consider to highlight the complexity of policy decisions on COVID-19 vaccination in this age group.”
The critical question for implementing any vaccine is:
“do the benefits of the vaccine in preventing the harms of the disease outweigh any known or potential risks associated with vaccination?”
“do the benefits of the vaccine in preventing the harms of the disease outweigh any known or potential risks associated with vaccination?”
U.S. proceeding with vaccinating children 5-11y based on Pfizer trial of 2x 10 µg doses in 2,268 children aged 5-11y showing vaccine:
• well tolerated
• induced robust neutralising antibody response.
• well tolerated
• induced robust neutralising antibody response.
Safety bar for vaccinating <12y needs to be high as direct risk from COVID is low:
• #COVID19 is asymptomatic or mild in vast majority
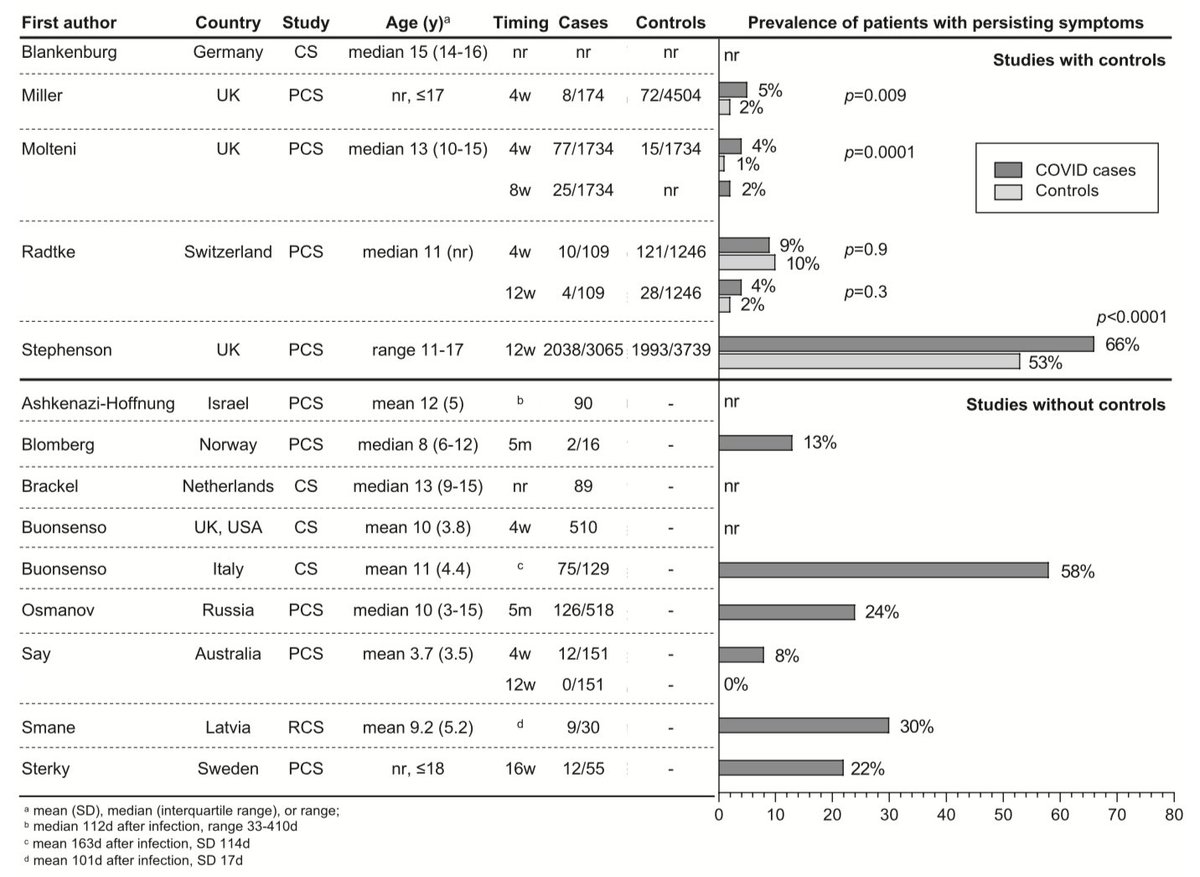
• #LongCOVID may not be as prevalent
• #MIS / PIMS-TS is rare; majority make rapid & full recovery.
• #COVID19 is asymptomatic or mild in vast majority
• #LongCOVID may not be as prevalent
• #MIS / PIMS-TS is rare; majority make rapid & full recovery.
Potential harms from COVID vaccination less well established in children <12y:
• Can’t extrapolate directly from adults: children’s immune response differs
• Pfizer trial (n=2,268 aged 5-11y) too small to detect rare adverse effects.
• Can’t extrapolate directly from adults: children’s immune response differs
• Pfizer trial (n=2,268 aged 5-11y) too small to detect rare adverse effects.
Best argument for vaccinating <12y might be to prevent population harms and indirect effects:
• Help reduce transmission
• Help keep schools open
Those at higher risk of severe COVID due to underlying conditions/comorbidities likely to have greatest benefit from vaccination.
• Help reduce transmission
• Help keep schools open
Those at higher risk of severe COVID due to underlying conditions/comorbidities likely to have greatest benefit from vaccination.
Coronavirus Infections in Children
bit.ly/3ol42o3
Why is COVID-19 less severe in children?
bit.ly/3qaHGIc
How Common Is Long COVID in Children?
bit.ly/3BLvEa
Should children be vaccinated against COVID-19?
bit.ly/2ZYyPi0
bit.ly/3ol42o3
Why is COVID-19 less severe in children?
bit.ly/3qaHGIc
How Common Is Long COVID in Children?
bit.ly/3BLvEa
Should children be vaccinated against COVID-19?
bit.ly/2ZYyPi0
• • •
Missing some Tweet in this thread? You can try to
force a refresh