
1) Welcome to a new #accredited #tweetorial on #hypertrophic #cardiomyopathy #HCM. Our expert author is Ahmad Masri MD @MasriAhmadMD of @OHSUCardio where he leads the Hypertrophic Cardiomyopathy Ctr. See a previous program from him, on #Fabry disease, at cardiometabolic-ce.com/cardiorenal-fa…. 

2a) This program is intended for #healthcare providers and is supported by an educational grant from Bristol-Myers Squibb. Statement of accreditation and faculty disclosures at cardiometabolic-ce.com/disclosures/. FOLLOW US for the most timely expert education in #cardiometabolic care!
2b) #Physicians #Nurses #PhysicianAssociates #NursePractitioners #Pharmacists earn a full 1⃣ hour of 🆓CE/#CME credit from following this 🧵. For educational purposes, Twitter still works!! 😁
3) #HCM is common, affects 1:200 to 1:500 adults in the US, and is a pan-ethnic disease without known sexual or racial predilections. Background:
👉🔓pubmed.ncbi.nlm.nih.gov/24998133/
👉🔓pubmed.ncbi.nlm.nih.gov/7641357/
👉🔓pubmed.ncbi.nlm.nih.gov/25814232/
Photo from nature.com/articles/nrcar…
👉🔓pubmed.ncbi.nlm.nih.gov/24998133/
👉🔓pubmed.ncbi.nlm.nih.gov/7641357/
👉🔓pubmed.ncbi.nlm.nih.gov/25814232/
Photo from nature.com/articles/nrcar…

4) #HCM is largely under-diagnosed. It is defined as maximal LV wall thickness of at least 15 mm (or 13-14 mm in the presence of family history) out of proportion to other comorbid conditions. #Echofirst is the primary tool used to diagnosed #HCM
See pubmed.ncbi.nlm.nih.gov/33229116/
See pubmed.ncbi.nlm.nih.gov/33229116/
5) There are different imaging phenotypes of #HCM which can be seen on #echofirst and/or #whycmr
Image from 🔓pubmed.ncbi.nlm.nih.gov/19589432/
Image from 🔓pubmed.ncbi.nlm.nih.gov/19589432/

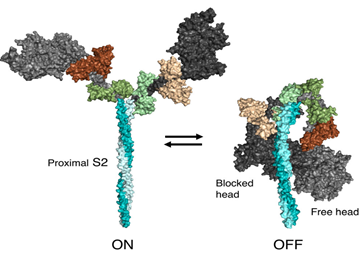
6) #HCM is a myocardial disease which results from a disordered hypercontractility state at the #sarcomere level. Normally, #actin and #myosin form cross-bridges which result in normal contractility and effective relaxation

7) However, myosin is not only bound to actin or available to bind, there is a third state called the super-relaxed state (off myosin) where the myosin head is folded inward and is not available to engage with actin.
See 🔓ncbi.nlm.nih.gov/pmc/articles/P…
See 🔓ncbi.nlm.nih.gov/pmc/articles/P…

8) In #HCM, hypercontractility is a central phenomenon of the disease. It was shown in 2000 in a mouse model of HCM (R403Q) that there is hypercontractility and excessive force generation.
👉pubmed.ncbi.nlm.nih.gov/10764406/
👉pubmed.ncbi.nlm.nih.gov/10764406/

9) This strong (or excessive) actin-myosin bound state leads not only to #hypercontractility, but also disordered relaxation (i.e. #diastole). See
👉🔓pubmed.ncbi.nlm.nih.gov/33983830/
👉🔓pubmed.ncbi.nlm.nih.gov/24655499/
👉🔓pubmed.ncbi.nlm.nih.gov/33983830/
👉🔓pubmed.ncbi.nlm.nih.gov/24655499/
10) Despite #HCM being a #sarcomere disease, traditional medical therapies to address the disease have not targeted the sarcomere, & invasive therapies are meant to anatomically modify the substrate
👉🔓pubmed.ncbi.nlm.nih.gov/31324451/
👉🔓pubmed.ncbi.nlm.nih.gov/31998849/
👉🔓pubmed.ncbi.nlm.nih.gov/31324451/
👉🔓pubmed.ncbi.nlm.nih.gov/31998849/


11) Cardiac #myosin inhibitors were invented to address the issue of hypercontractility at the #sarcomere level without affecting calcium currents in myocytes.
12) Back to the myosin state, the goal in #HCM would be to increase the super-relaxed state of #myosin where it is unavailable to engage with #actin. See
👉🔓pubmed.ncbi.nlm.nih.gov/28717924/
👉🔓pubmed.ncbi.nlm.nih.gov/28223517/
👉🔓pubmed.ncbi.nlm.nih.gov/30104387/
👉🔓pubmed.ncbi.nlm.nih.gov/28717924/
👉🔓pubmed.ncbi.nlm.nih.gov/28223517/
👉🔓pubmed.ncbi.nlm.nih.gov/30104387/
13) The first cardiac myosin inhibitor (#CMI) was #mavacamten; in an animal model of #HCM, it increases the super-relaxed state (#SRX) of myosin. See
👉🔓pubmed.ncbi.nlm.nih.gov/28717924/
👉🔓pubmed.ncbi.nlm.nih.gov/28223517/
👉🔓pubmed.ncbi.nlm.nih.gov/30104387/
👉🔓pubmed.ncbi.nlm.nih.gov/28717924/
👉🔓pubmed.ncbi.nlm.nih.gov/28223517/
👉🔓pubmed.ncbi.nlm.nih.gov/30104387/

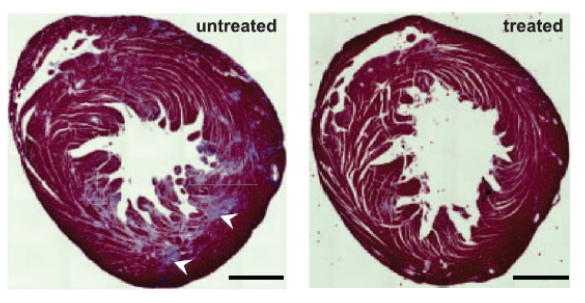
14) #Mavacamten has also been shown to prevent hypertrophy, reduce myocyte disarray, and reduce #fibrosis in animal models of #HCM. See 🔓pubmed.ncbi.nlm.nih.gov/26912705/


15) Tying it all together – cardiac myosin inhibitors represent the first class of medications to directly address the underlying #pathophysiology of #HCM
👉 🔓pubmed.ncbi.nlm.nih.gov/31324451/
👉 🔓pubmed.ncbi.nlm.nih.gov/31324451/

16) In addition to these manifestations, there are monogenic causes of #HCM with complex genetic basis of the disease. The two most common gene mutations occur in #MYBPC3 and #MYH7
See 🔓pubmed.ncbi.nlm.nih.gov/28007147/
See 🔓pubmed.ncbi.nlm.nih.gov/28007147/

17) Another way to think about this is an imbalance between the gas and the brake mechanism. #MYH7 represents the gas (too much of it) while #MYBPC3 represents the brake (too little of it), and why those variants can cause #HCM
🔓pubmed.ncbi.nlm.nih.gov/28007147/
🔓pubmed.ncbi.nlm.nih.gov/28007147/
18) While genetic basis of the disease and genetic variants are extremely important in #HCM, they only explain 40-50% of the cases seen and are associated with worse outcomes as shown in the #SHaRe registry
👉🔓pubmed.ncbi.nlm.nih.gov/30297972/
👉🔓pubmed.ncbi.nlm.nih.gov/30297972/

19) Back to disease classification: for tx decisions, #HCM is obstructive (#HOCM) or non-obstructive #HCM. This is based on having LV outflow tract (#LVOT) gradient of at least 30 mmHg as a result of systolic anterior motion of the mitral valve (#SAM).
See pubmed.ncbi.nlm.nih.gov/33229116/
See pubmed.ncbi.nlm.nih.gov/33229116/

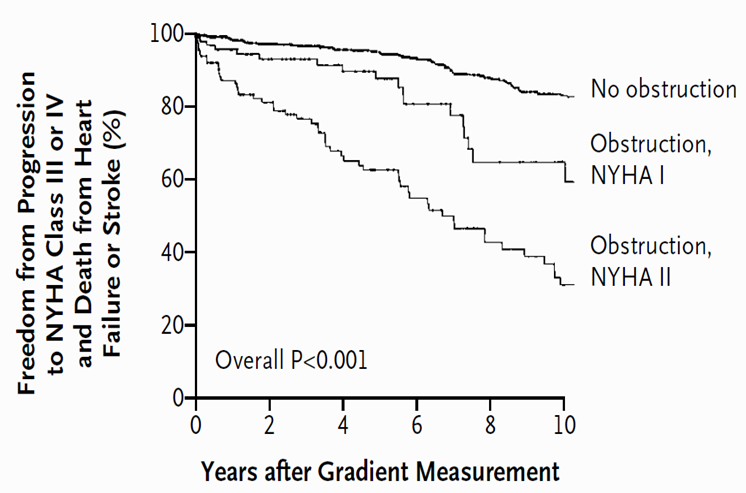
20) Why is defining #SAM and #LVOT_obstruction important? First, for treatment purposes and second, because it relates to #prognosis.
See 🔓pubmed.ncbi.nlm.nih.gov/12540642/
See 🔓pubmed.ncbi.nlm.nih.gov/12540642/

21) In terms of treatment, the whole therapeutic approach in #HCM relies on this classification, where it is estimated that 2/3 of #HCM patients are obstructive (at rest or with provocation)
pubmed.ncbi.nlm.nih.gov/33215931/
pubmed.ncbi.nlm.nih.gov/33215931/
22) The classification drives therapies to improve quality of life (QoL) in patients with #HCM. By intervening on those with #LVOT obstruction, a proportion remain with diastolic dysfunction and behave similar to non-obstructive HCM

23) Patients are typically started on #beta_blockers or #calcium_channel_blockers, and if they remain with significant symptoms, then they are typically offered second line therapies or invasive intervention.
24) The other therapeutic focus is risk stratifying patients for sudden cardiac death #SCD and the use of implantable cardioverter defibrillator (#ICDs)
pubmed.ncbi.nlm.nih.gov/33229116/
pubmed.ncbi.nlm.nih.gov/33229116/

25) The use of #ICDs with modern therapy in #HCM led to improvement in survival, but this meant that the lifetime risk of heart failure and arrhythmias would have ⬆️ in this population
pubmed.ncbi.nlm.nih.gov/30297972/
pubmed.ncbi.nlm.nih.gov/30297972/

26) And the natural history of #HCM aside from sudden cardiac death is influenced by degree of obstruction, symptoms, and treatment.
🔓pubmed.ncbi.nlm.nih.gov/12540642/
🔓pubmed.ncbi.nlm.nih.gov/12540642/
27) With septal myectomy, ICDs and other interventions, outcomes of symptomatic obstructive #HCM appear to be favorable
🔓pubmed.ncbi.nlm.nih.gov/25953744/
🔓pubmed.ncbi.nlm.nih.gov/25953744/

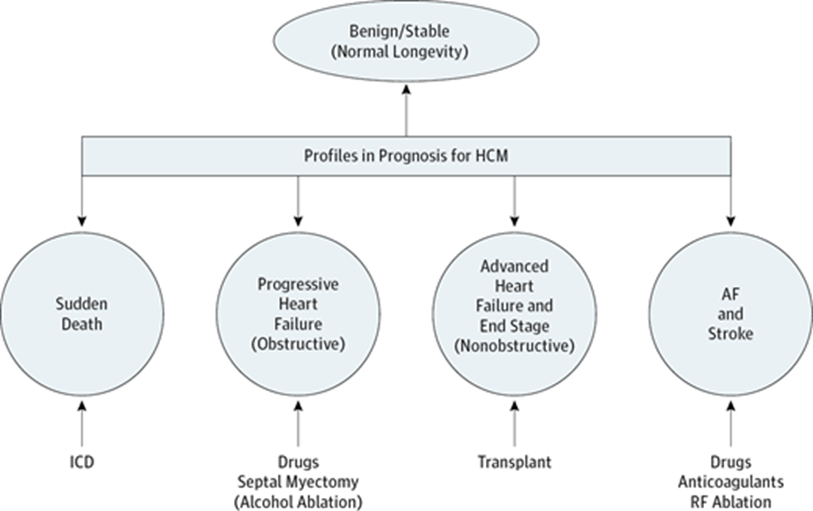
28) However, there remain challenges in the care of patients with #HCM, and they can be profiled into these groups, where #heartfailure and #arrhythmias represent a major unmet need
pubmed.ncbi.nlm.nih.gov/27437663/
pubmed.ncbi.nlm.nih.gov/27437663/
29) Up until recently, all therapies used in #HCM lacked any robust large multicenter trial data to support their use. #Mavacamten, a cardiac myosin inhibitor which is now approved by @US_FDA, is the first one with such data.
30) We'll pick up this 🧵tomorrow! Meanwhile, a knowledge ✔️:
Which of the following 💊is NOT a primary treatment in medical management of obstructive #HCM?
MARK YOUR CHOICE!
a. beta blockers
b. dihydropyridine CCB
c. nondihydropyridine CCB
d. disopyrimide
Which of the following 💊is NOT a primary treatment in medical management of obstructive #HCM?
MARK YOUR CHOICE!
a. beta blockers
b. dihydropyridine CCB
c. nondihydropyridine CCB
d. disopyrimide
31) Welcome back to our #accredited #tweetorial on #HCM! I am @MasriAhmadMD and you are earning 1⃣ hour 🆓CE/#CME credit! Follow @cardiomet_CE to address your CE needs with expert-authored programs delivered entirely on Twitter!
32) Yesterday's quiz (tweet 30)? In obstructive #HCM we avoid meds that ⬇️ventricular preload and thus ⬆️flow obstruction. These include dihydropyridine #CCBs, nitroglycerin, #ACEi (all ⬇️systemic vascular resistance), & diuretics, which ⬇️blood delivery to the 🫀. B is correct!
33) So yesterday we started talking about #mavacamten, which was approved on the basis of the #EXPLORER_HCM trial ➡️20% difference in a co-primary endpoint (PVO2 and NYHA class) between the mavacamten arm and placebo over a 30 week treatment period
See pubmed.ncbi.nlm.nih.gov/32871100/
See pubmed.ncbi.nlm.nih.gov/32871100/


35) #Mavacamten also showed marked improvement in patient reported outcomes (by #KCCQ, available at 🔓aci.health.nsw.gov.au/__data/assets/…).
See pubmed.ncbi.nlm.nih.gov/34004177/
See pubmed.ncbi.nlm.nih.gov/34004177/

36) #Mavacamten improved markers of diastolic function as well. This occurred over a 30 week period in those with obstructive HCM #HOCM
See pubmed.ncbi.nlm.nih.gov/34915982/
See pubmed.ncbi.nlm.nih.gov/34915982/

37) #Mavacamten was associated with some events of low #LVEF, for which the majority were asymptomatic and are reversible with reducing the dose/withdrawal of treatment. LVEF decrease is discrepant with other markers.

38) This #LVEF reduction with treatment is distinct from the natural history of untreated #HCM, where LVEF<50% reflects a burnt-out fibrotic stage associated with significant mortality and morbidity
👉🔓pubmed.ncbi.nlm.nih.gov/32228044/
👉🔓pubmed.ncbi.nlm.nih.gov/32553256/
👉🔓pubmed.ncbi.nlm.nih.gov/32228044/
👉🔓pubmed.ncbi.nlm.nih.gov/32553256/


39) @US_FDA approved #mavacamten on the basis of #EXPLORER_HCM trial. However, due to the risk of LV systolic dysfunction, narrow therapeutic window, and potential drug-drug interactions, the FDA mandated a sophisticated REMS program
40) REMS = an FDA program titled "Risk Evaluation and Mitigation Strategy" which aims to ensure that effective medications with safety concerns have a pathway – read more here
fda.gov/drugs/drug-saf….
fda.gov/drugs/drug-saf….
41) As part of the #REMS program, prescriber, patient and pharmacy have to enroll, and the drug can be dispensed only if all the established rules are satisfied
Read more here if interested: camzyosrems.com/healthcare-pro…
Read more here if interested: camzyosrems.com/healthcare-pro…
42) The initiation phase is shown below – this is the first time you would see the cut-off of 20 mmHg for LVOT gradient being used. This is used to consider patients who drop to below 20 mmHg within 4 weeks as “super responders” and that it is safer to down-titrate to 2.5 mg.

43) Patients must stay on the same dose for 12 weeks, & have 3 echo's during this time, before up-titration can occur. If they had 2 echo's with Valsalva LVOT gradient < 20 mm Hg, then the drug should be withheld.
44) After the 12 weeks, every dose titration requires an echo follow up after 4 weeks and dose maintained for at least another 8 weeks, and then routinely, echo follow-up should be done once every 3 months

45) Patients must be reminded of drug-drug interactions, and the medications need to be reconciled when #mavacamten is dispensed. Some of the medications that interact are #OTC (omeprazole) but some are Rx for acute treatment (Paxlovid).
46) Patients also have to be on a highly reliable form of contraception to be on mavacamten. This presents challenges in the younger population of patients with obstructive #HCM.
47) #Mavacamten has only been approved for patients with obstructive #HCM, #NYHA class II-III, on standard background first line medical therapy for obstructive #HCM. It is not approved for asymptomatic or non-obstructive HCM.
48) #Mavamcaten cost + resource utilization/cost of monitoring remain issues that require further evaluation, which is underway.
49) So . . . back to the #mavacamten trial data. In #EXPLORER, 2/3 of patients were #NYHA class II, and if patients require septal reduction therapy within the trial duration, they were excluded.
50) A second phase 3 trial, #VALOR_HCM (presented at #ACC22), recruited patients who were referred to septal reduction therapy based on symptoms (typically NYHA class III/IV) + obstructive LVOT gradient > 50 mm Hg.
See acc.org/Latest-in-Card….
See acc.org/Latest-in-Card….
51) VALOR-HCM recruited 112 patients referred for septal reduction therapy, with placebo controlled trial for 16 weeks followed by dose blinded cross over from placebo to #mavacamten.

52) #VALOR was not a head-to-head trial of #mavacamten vs #myectomy. Rather, the goal was to show if mavacamten works well in a septal reduction therapy population, and if its use might avert the need for septal reduction therapy.
53) The primary outcome was met as shown with 82% of patients on mavacamten being guideline-ineligible for septal reduction therapy at week 16.
See acc.org/Latest-in-Card….
See acc.org/Latest-in-Card….

55) The Week 32 data were presented at #AHA22 and published as well, showing similar efficacy profile, but a high rate of low LVEF events (12.5% in the #mavacamten group and 5.7% in the placebo-mava group).
See abstract 🔓ahajournals.org/doi/10.1161/CI…
See abstract 🔓ahajournals.org/doi/10.1161/CI…

56) #Atrial_fibrillation was seen in 3 patients (5.4%) of the #mavacamten group over 32 weeks. None occurred in placebo-to-mava group. No details if these patients had hx of PAF or not. One patient with LVEF < 30% + Afib had permanent d/c of mava with return to baseline #LVEF.
57) #Mavacamten was also evaluated for safety and dose finding in non-obstructive HCM (#nHCM) in the phase II #MAVERICK_HCM trial.
See 👉pubmed.ncbi.nlm.nih.gov/32466879/.
See 👉pubmed.ncbi.nlm.nih.gov/32466879/.

58) MAVERICK-HCM showed that #mavacamten was generally well tolerated, and reduced markers of wall stress (#NTproBNP) and subclinical myocardial injury (#troponin).

59) The incidence of low LVEF was 12.8% in the study. This is generally reversible and not known to be associated with long term adverse outcomes.
60) #MAVERICK_HCM informed the design of the upcoming/soon to enroll #ODYSSEY_HCM trial, a phase III trial of #mavacamten in #nHCM
clinicaltrials.gov/ct2/show/NCT05…
clinicaltrials.gov/ct2/show/NCT05…
61) Finally, patients who received #mavacamten as part of #EXPLORER and #MAVERICK were enrolled in the #MAVA_LTE trial, which is a 5 year long term open-label extension study. Overall, mavacamten continued to have a similar efficacy profile to those seen in the parent studies.

62) In terms of safety, outcomes were similar to the obstructive cohort, but there was a higher rate of low LVEF events in the #nHCM cohort. See 🔓abstract at ahajournals.org/doi/abs/10.116….

63) Aside from #mavacamten, another cardiac myosin inhibitor is in development & undergoing clinical trials. #Aficamten has a similar therapeutic MoA but different binding site.
See 🔓 pubmed.ncbi.nlm.nih.gov/34627791/
🔓 pubmed.ncbi.nlm.nih.gov/34606259/
See 🔓 pubmed.ncbi.nlm.nih.gov/34627791/
🔓 pubmed.ncbi.nlm.nih.gov/34606259/
64) We'll discuss that agent and wrap up this program tomorrow--be sure to return and claim your 1⃣ hour🆓CE/#CME!
👏to @ValleAlfonso @hvanspall @DrMarthaGulati @SeguraCardio @DavidFerminMD @DesaiMilindY @CSHeartResearch @HanCardiomd @SABOURETCardio
👏to @ValleAlfonso @hvanspall @DrMarthaGulati @SeguraCardio @DavidFerminMD @DesaiMilindY @CSHeartResearch @HanCardiomd @SABOURETCardio
65) Welcome back! You are > 2/3 done earning 1⃣ full hour of 🆓CE/#CME right here on Twitter, at your best source for #cardiometabolic education! Expert faculty @MasriAhmadMD is teaching us all about the course of #HCM and new/evolving medical mgt options.
66) Yesterday we introduced a cardiac #myosin inhibitor in development, #aficamten. This drug has a shorter half life than #mavacamten, a wide therapeutic window, and no known drug-drug interactions
See 🔓pubs.acs.org/doi/full/10.10…
See 🔓pubs.acs.org/doi/full/10.10…


67) The first phase II trial of #aficamten was in obstructive #HCM patients and called the #REDWOOD_HCM trial (Cohorts 1 and 2). In Cohort 1, dose was 5-15 mg, and 10-30 mg in Cohort 2.
See nonaccredited 📽️at practicalcardiology.com/view/understan…
See nonaccredited 📽️at practicalcardiology.com/view/understan…

68) REDWOOD-HCM Cohorts 1 and 2 trial showed rapid and sustained reduction in #LVOT gradients, and the safety of using aficamten. Aficamten also had a high hemodynamic response and improvement in #NYHA class


69) There were 2 events of low #LVEF. Both happened with the higher dose rapid titration strategy(going from 10 to 20 mg aficamten). This informed the design of the ongoing phase III SEQUOIA-HCM trial.
clinicaltrials.gov/ct2/show/NCT05…
clinicaltrials.gov/ct2/show/NCT05…
70) SEQUOIA-HCM is a 270 patient trial (largest obstructive #HCM trial to date), enrolling patients with obstructive #HCM and #NYHA class II/III. Dose range is 5-20 mg.

71) Back to #REDWOOD, there was a 3rd Cohort of patients with obstructive #HCM refractory to an AV nodal blocking agent + #disopyramide.
Abstract 🔓jacc.org/doi/10.1016/S0…
Abstract 🔓jacc.org/doi/10.1016/S0…

72) #Aficamten was added in an open label fashion with a dose range of 5-15 mg, showing 1) safety of 3 negative inotropes 2) no QT prolonging properties/interaction and 3) 3/4th of patients had improvement in their #LVOT obstruction.


74) All subjects who received aficamten in REDWOOD-HCM and SEQUOIA-HCM will be allowed to roll over to a 5 year long term extension study called FOREST-HCM (formerly REDWOOD-OLE). 73) See 📽️at esc365.escardio.org/presentation/2…



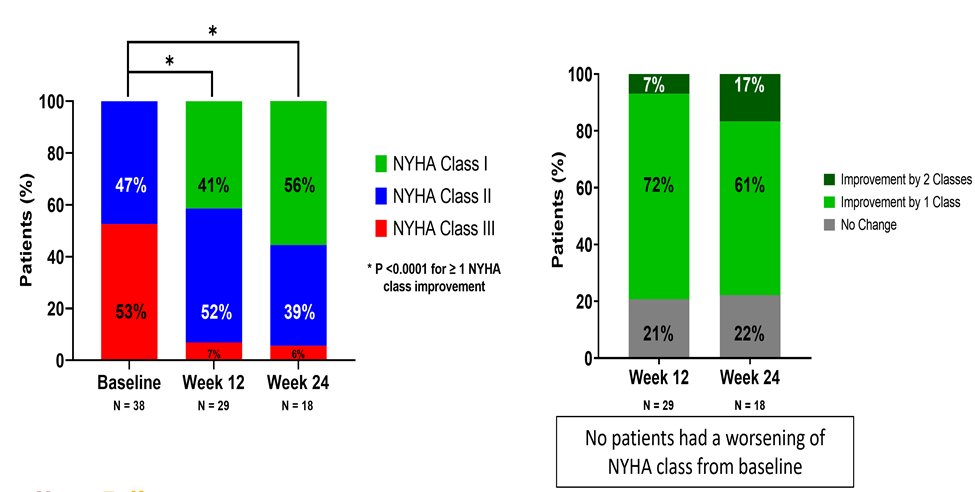
76) #Aficamten was also associated with improvement in #KCCQ-OS in FOREST-HCM (REDWOOD-OLE)
See 📽️at cfrjournal.com/video-index/hf….
See 📽️at cfrjournal.com/video-index/hf….


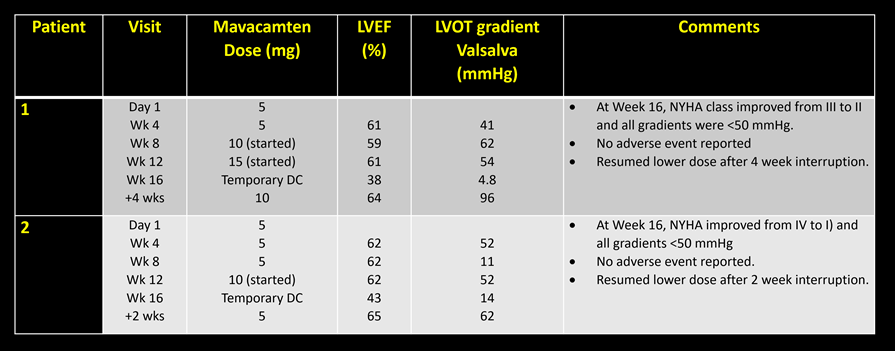
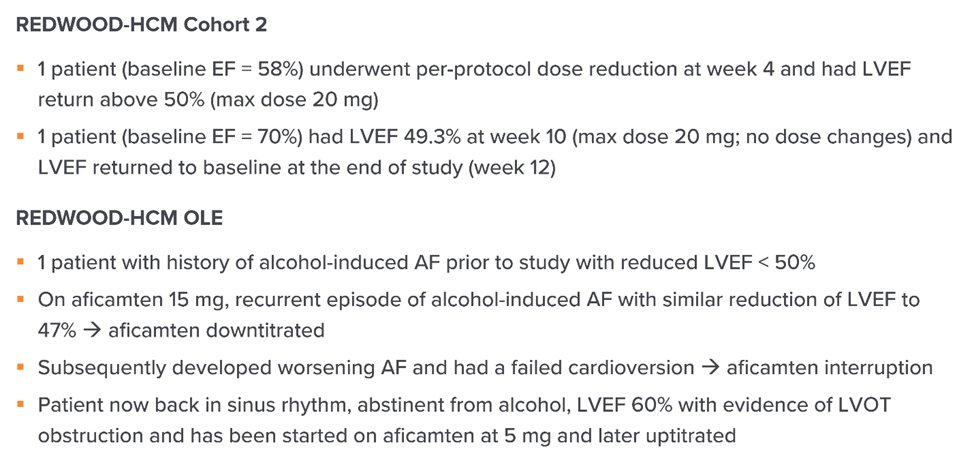
77) This is a summary of the confirmed low LVEF events in REDWOOD-HCM and REDWOOD-OLE (FOREST-HCM)
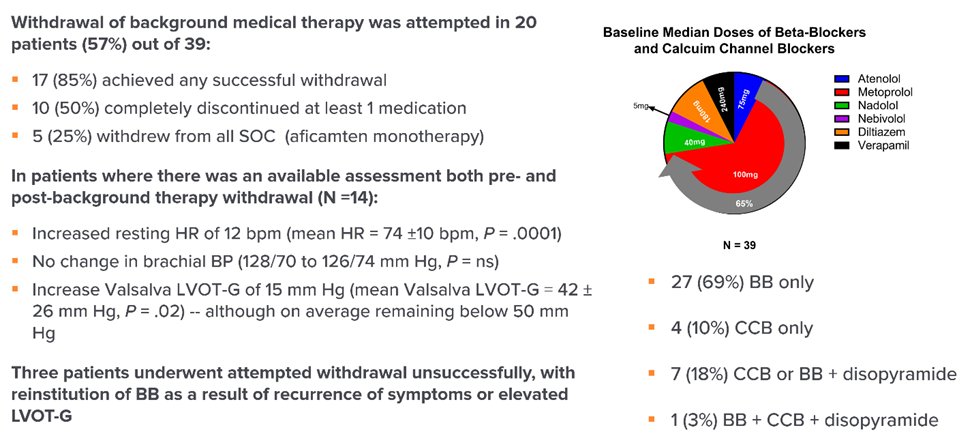
78) Another study from FOREST-HCM evaluated withdrawal of background medical therapy once on a stable dose of aficamten, showing its feasibility and safety. See more details at ir.cytokinetics.com/news-releases/…
79) Currently, a 2nd phase III trial of aficamten in #HOCM is planned to start soon: aficamten vs metoprolol, head to head, using #CPET. This would be the first evaluation of metoprolol using CPET in a large multicenter trial in obstructive #HCM. The trial is called MAPLE-HCM.

80) Another recent trial was the TEMPO HCM trial, which was the first trial to evaluate metoprolol/BB in obstructive HCM, while BB have been used since the 1960s
81) This trial showed improvement in symptoms and #LVOT gradients but no difference in pVO2, #NTproBNP, and only a 3 point difference in #KCCQ. See pubmed.ncbi.nlm.nih.gov/34915981/.


82) Starting to wind down now, this is an example of a patient with #HOCM who has been doing well for years on #mavacamten, with significant reverse remodeling

83a) And here is the follow up video at Week 144. Evidence of the reverse #remodeling seen with improved #LVOT gradient and markers of diastolic function, indicating both reverse remodeling and improved cardiac structure.
83b) And more from the "post" visit . . .

84) And here is an example of using #aficamten as part of a clinical trial in someone with significant #SAM but without severe hypertrophy (15 mm), and symptoms refractory to medical therapy:
https://twitter.com/MasriAhmadMD/status/1469824288899276808?s=20&t=p1Z6R1XKElnx_IEeZWIkew
85a) What is the indication for treating patients with obstructive HCM ?
A) LVOT gradient > 100 mmHg at rest
B) Symptoms either at rest or with exertion
C) To decrease left atrial size index
D) To prevent future heart failure hospitalization
A) LVOT gradient > 100 mmHg at rest
B) Symptoms either at rest or with exertion
C) To decrease left atrial size index
D) To prevent future heart failure hospitalization
85b) The correct Answer is B – the treatment goal is to relieve symptoms
86a) In which of the following cases should #mavacamten NOT be used?
A) Obstructive HCM with an LVOT gradient of 70 mmHg and NYHA class II
B) Symptomatic obstructive HCM with an LVOT gradient of 52 mmHg 1 year after septal myectomy
(cont)
A) Obstructive HCM with an LVOT gradient of 70 mmHg and NYHA class II
B) Symptomatic obstructive HCM with an LVOT gradient of 52 mmHg 1 year after septal myectomy
(cont)
(cont--mark your response below)
C) Symptomatic obstructive HCM with 5 mmHg LVOT gradient at rest which increases to 83 mmHg with Valsalva
D) Symptomatic HCM with an LVEF of 48%
C) Symptomatic obstructive HCM with 5 mmHg LVOT gradient at rest which increases to 83 mmHg with Valsalva
D) Symptomatic HCM with an LVEF of 48%
86b) The correct answer is D – #mavacamten is not to be used in patients with systolic dysfunction.
87) Finally, treatment of patients with obstructive #HCM is rapidly evolving. Evidence-based medicine is transforming HCM, and randomized clinical trials should be considered in every patient. Shared decision making is central in the treatment of patients with HCM!

88) And you have just completed 1⃣ hour of CE/#CME! Claim your certificate 🇺🇸🇨🇦🇪🇺🇬🇧 at cardiometabolic-ce.com/HCM1/ and FOLLOW US for more expert education on #HCM and other #cardiometabolic disease! I am @MasriAhmadMD.
#FOAMed #cardiotwitter #MedTwitter @MedTweetorials
#FOAMed #cardiotwitter #MedTwitter @MedTweetorials
• • •
Missing some Tweet in this thread? You can try to
force a refresh











