Using health data to learn what works.
Making #causalinference less casual.
Director @CAUSALab | Professor @HarvardChanSPH | Methods Editor @AnnalsofIM
 2/
2/ 2/
2/ 2/
2/


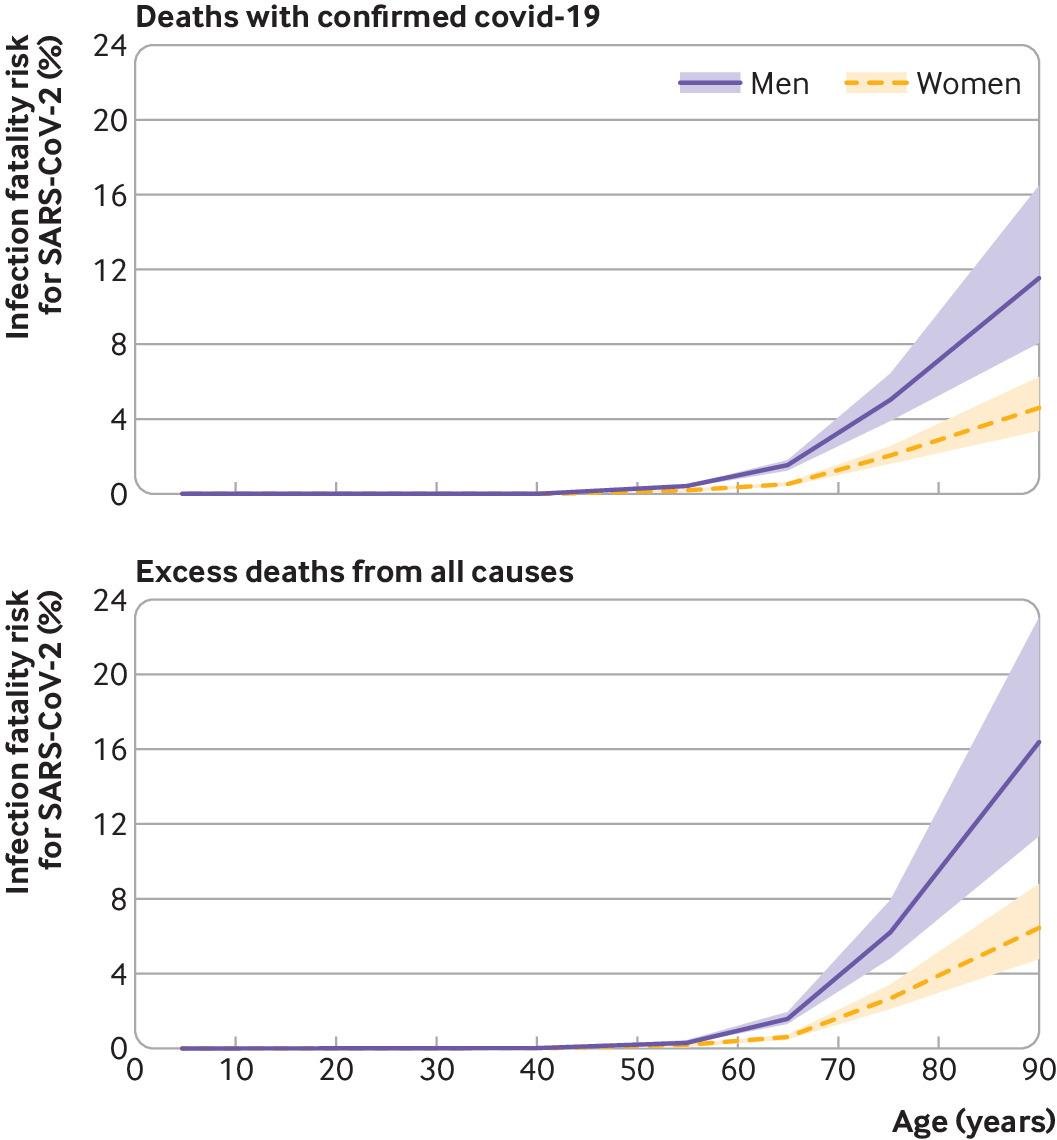 2/ The IFR in a population is the ratio of
2/ The IFR in a population is the ratio of 2/ Porque:
2/ Porque: 2/
2/ 2/
2/ That is, individuals on TDF/FTC had about half the risk of #COVID19 hospitalization than those on TAF/FTC or ABC/3TC.
That is, individuals on TDF/FTC had about half the risk of #COVID19 hospitalization than those on TAF/FTC or ABC/3TC.
 @xabieradrian @AnnalsofIM @HarvardEpi @harvard_data @HarvardBiostats @HarvardChanSPH @CMSGov @CMSgovPress @MonganInstitute @MassGeneralNews 2)
@xabieradrian @AnnalsofIM @HarvardEpi @harvard_data @HarvardBiostats @HarvardChanSPH @CMSGov @CMSgovPress @MonganInstitute @MassGeneralNews 2)
 2/
2/