Interesting case presentation today @ellamimasamayor of a 20 yo, female, with an episode of hematemesis. EGD done revealed H. pylori +, duodenal ulcers. CT scan showed pancreatic head mass. Referred due to elevated blood pressure, recurrent hypokalemia and blurring of vision.
BP
Upper Ext - R 200/120. L 160/100
Lower Ext - R 160/100. L 170/100
PE did not show cushingoid features. CV exam showed decreased pulses on the left arm. Rest was unremarkable
Upper Ext - R 200/120. L 160/100
Lower Ext - R 160/100. L 170/100
PE did not show cushingoid features. CV exam showed decreased pulses on the left arm. Rest was unremarkable

Fundoscopy showed
OD: clear media, grade 4 papilledema, hard exudates with exudative retinal detachment
OS: grade 1 papilledema
OD: clear media, grade 4 papilledema, hard exudates with exudative retinal detachment
OS: grade 1 papilledema
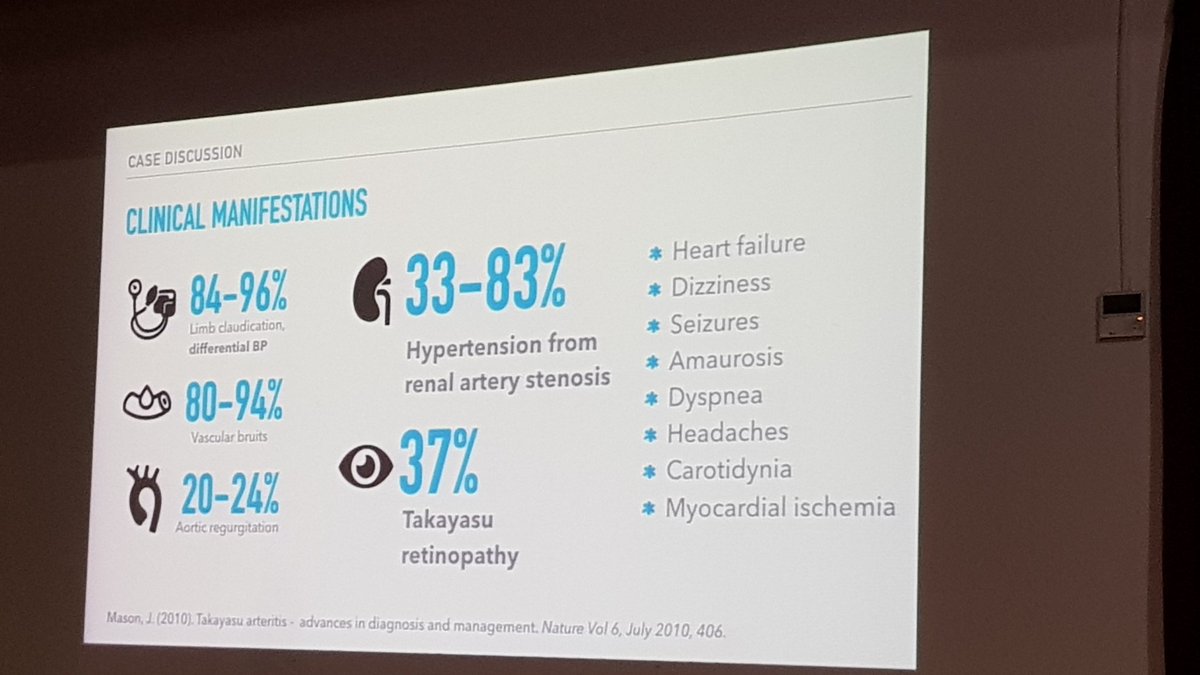
Secondary hypertension in emergency, considerations
1. large vessel vasculitis
2. pancreatic neuroendocrine tumor
3. primary hyperaldosteronism
4. renal artery stenosis
5. pheochromocytoma vs paranganglioma
HTN retinopathy
H. pylori infection with erosive gastropathy
1. large vessel vasculitis
2. pancreatic neuroendocrine tumor
3. primary hyperaldosteronism
4. renal artery stenosis
5. pheochromocytoma vs paranganglioma
HTN retinopathy
H. pylori infection with erosive gastropathy
Hyperreninemic hyperaldosteronism
Urine metanephrines are only 1.3 ro 3x elevated
Urine metanephrines are only 1.3 ro 3x elevated

CV workup
ECG: sinus rhythm left atrial abnormality, left ventricular hypertrophy
Echo: 55% EF, concentric LVH, segmental wall hypokinesia (inferoseptal)
Arterial Duplex: upper extremities mild stenosis left midsubclavian artery, lower extremities normal ADS
ECG: sinus rhythm left atrial abnormality, left ventricular hypertrophy
Echo: 55% EF, concentric LVH, segmental wall hypokinesia (inferoseptal)
Arterial Duplex: upper extremities mild stenosis left midsubclavian artery, lower extremities normal ADS
Here is when it gets interesting. Stenosis were noted on the R common carotid, R subclavian

as well as stenosis on the left subclavian artery

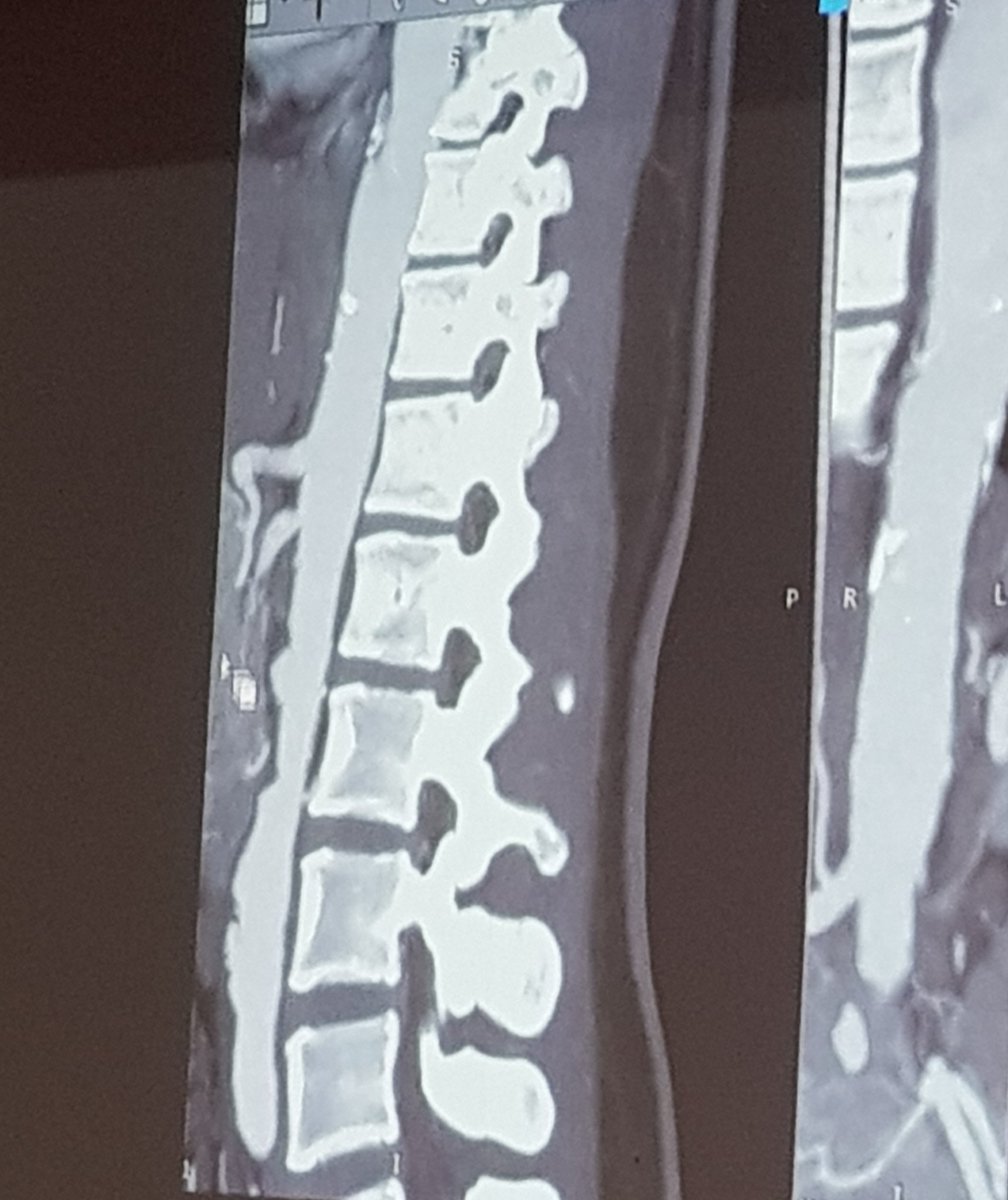
Stenosis and total cutoff of the contrast on the left renal artery with a relatively smaller kidneys on the left.

The sagital view of the aorta shows multiple outpoutchings from the lumen indicative of accelerated atherosclerosis and possibly stenosed segments.
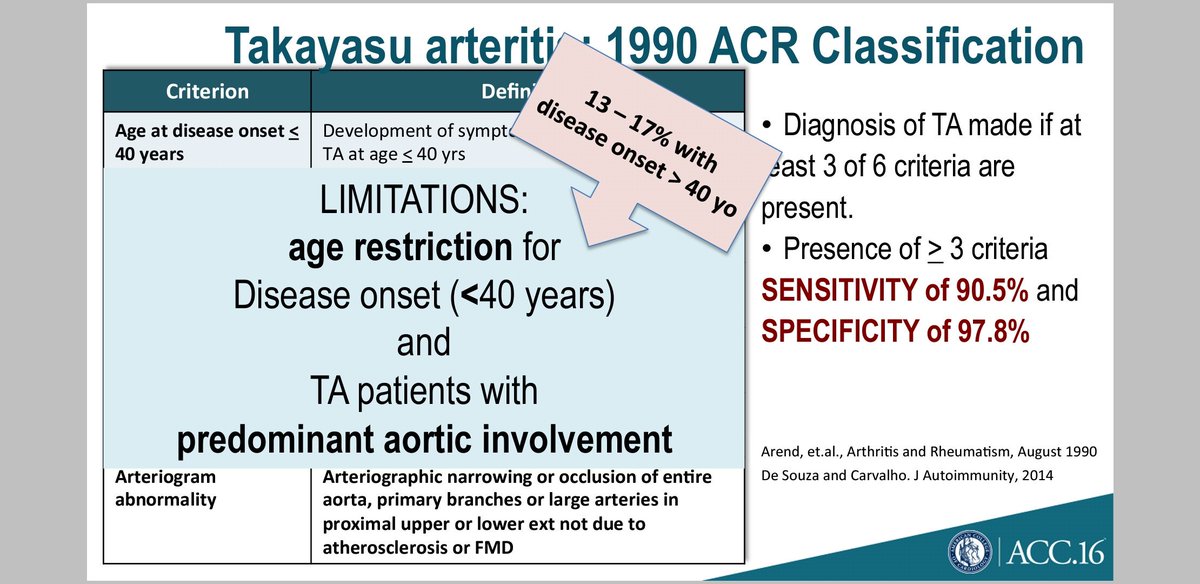
Based on the ACR criteria, the patient satisfied 4/6 for Takayasu arteritis.

Takayasu arteritis involving the L renal a, B subclavian a, R common carotid a, SMA with secondary HTN. A beautiful demonstration of Occam's razor the principle of parsimony.
Of note: the pancreatic head mass was not consistent with PNET since it had minimal enhancement on CT. PNETs are usually highly vascular tumors.

Important take home point from @doktora_ging that Takayasu arteritis can present in ages above >40 years old. Slide from Dr. Abola
Filipino demographics of Takayasu arteritis by the study done by Abola et al still shows female preponderance with >20% incidence in age>40
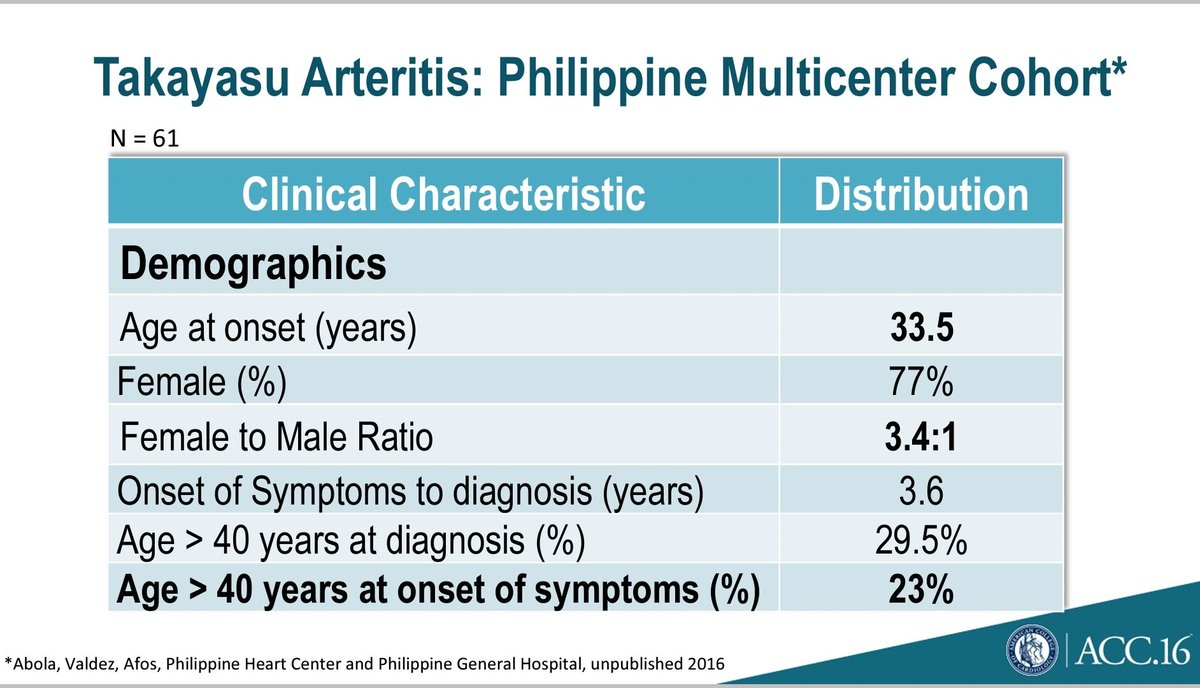
Hypertension, visual disturbances and aortic aneurysms were the MC presentations/ complications

Type V distribution of arterial lesions is the predominant type in contrast to type I-IIa in Japanese and USA patients


This patient was successfully treated with prednisone and methotrexate and was sent home.
When to consider surgery and what is the prognosis?

Error: urine metanephrines were only 1.3 to 2x elevated.