Let's get started on our first @realbrainbook CBD.
A 49 year old woman presents to the emergency department with an acute onset headache, vomiting, neck stiffness and photophobia. On examination she is conscious and alert with a GCS of 15. She has no neurological deficits #BBSAH
A 49 year old woman presents to the emergency department with an acute onset headache, vomiting, neck stiffness and photophobia. On examination she is conscious and alert with a GCS of 15. She has no neurological deficits #BBSAH
Based on the history what are your thoughts on differential diagnoses? #BBSAH
Indeed, some great differentials mentioned. Here are some important ones to consider:
Vascular: Ruptured #aneurysm, Ruptured arterio-venous malformation #AVM
Infectious: #Meningitis ,Ruptured mycotic aneurysm
Other: #Migraine, Traumatic haemorrhage #BBSAH
Vascular: Ruptured #aneurysm, Ruptured arterio-venous malformation #AVM
Infectious: #Meningitis ,Ruptured mycotic aneurysm
Other: #Migraine, Traumatic haemorrhage #BBSAH
Now that you have a few differentials in mind you go onto try and obtain some more information. What questions would you like to ask? #BBSAH
Any thoughts? Any red flag symptoms you want to ask about?
She reports the headache is located at the occiput and radiates to her forehead. This is the worst headache she has experienced. She also states she has a history of hypertension and is a smoker. #BBSAH
With this information in mind, now what do you think is the top differential? #BBSAH
Some really great thoughts on the top differential so far. Now that you have your differential in mind, what would you like to do next and why? #BBSAH
A non-contrast CT head is done and is shown below. In a CT head scan blood appears as white (below). Describe what you see. #BBSAH 
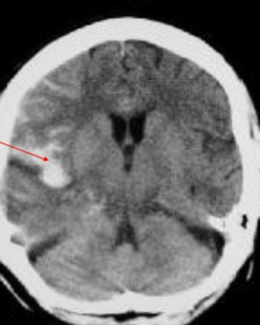
The CT head confirms a sub-arachnoid haemorrhage in the right sylvian fissure. CT head scans are frequently the first imaging test performed in SAH. It will identify over 95% of SAH if scanned in the first 48 hours. #BBSAH
If the CT scan is negative, does anyone know of any other tests we can do? #BBSAH
If the CT head is negative, a lumbar puncture (LP) can be performed. An LP is a sensitive test for SAH and is ideally performed 12 hours after the headache onset. Do you know why that is?
Great answers here. The reason for the 12 hours time is to allow for the development of xanthochromia.
Xanthochromia is a yellow discolouration of the CSF. This happens because of the breakdown of red blood cells which release haem pigments. This test is also useful because it helps differentiate a SAH from a traumatic tap (when the needle enters an epidural vein during LP)#BBSAH
This is what xanthochromia looks like.

So now that we’ve diagnosed a SAH, we need to identify the source. To do this a CT angiography (CTA) is carried out. This involves injecting contrast into a vein usually in the arm and allows us to visualise blood flow in the arterial vessels in the brain. #BBSAH
CTA is a really useful test because not only does it help us identify the source of the bleed, but it also demonstrates the vascular anatomy and the relation to nearby bony structures. This is important for surgical planning. #BBSAH
The CTA demonstrates an aneurysm in the middle cerebral artery (MCA). This is one of the most common arteries involved along with anterior communicating artery and posterior communicating artery.

The middle cerebral artery arises from the internal carotid artery and is divided into 4 segments (M1-M4). MCA aneurysms most commonly occur in the M1segment. The M1 segment travels horizontally from the internal carotid artery bifurcation to the bifurcation at the insula.

Aneurysms are pathologic dilatations in the wall of blood vessels. These areas bulge out and fill with blood. Aneurysms typically form at the branch points of arteries. This is because these tend to be the weakest areas. #BBSAH
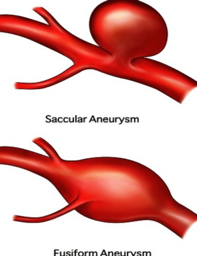
What types of brain aneurysms do you know? #BBSAH
Aneurysms can either be saccular or fusiform in shape. Fusiform shaped aneurysms bulge out on all sides of the blood vessels. Saccular (berry) aneurysms bulge out on only one side. These are the most common type. #BBSAH
As well as shape, aneurysm’s can also be split into size. They can be classified as small (<10mm), large (10-24mm) or giant (>24mm). #BBSAH
Over time the aneurysms weaken and can rupture. When it ruptures, the blood extravasates into the subarachnoid space. This is the space between the arachanoid membrane and the pia mater. This is why we call it a SAH.

SAH typically presents with the sudden onset of a severe headache, vomiting, neck pain (from meningeal irritation) and photophobia. Symptoms very similar to how our patient presented. In severe cases however patients may be unconscious.
There are a number of causes of SAH. The most common cause is trauma. SAH can also occur from a ruptured intracranial aneurysm, cerebral arterio-venous malformation or from coagulation disorders. #BBSAH
There are also a number of risk factors for SAH too. Can anyone identify any risk factors in our patients history and any other risk factors causing SAH? #BBSAH
Indeed, smoking and hypertension.Others include:
Trauma
Known arterio-venous malformation
Gender and age (higher in women, average age of onset >50y/o)
Alcohol abuse
Hereditary – Ehlers Danlos (type IV), autosomal dominant polycystic kidney disease, Osler-Weber-Rendu syndrome
Trauma
Known arterio-venous malformation
Gender and age (higher in women, average age of onset >50y/o)
Alcohol abuse
Hereditary – Ehlers Danlos (type IV), autosomal dominant polycystic kidney disease, Osler-Weber-Rendu syndrome
Let’s go onto the treatment options now. Assessment of the patient’s condition after a SAH is of the utmost importance and crucial to further management. There are a number of grading scales used which can determine the severity and help predict the prognosis.
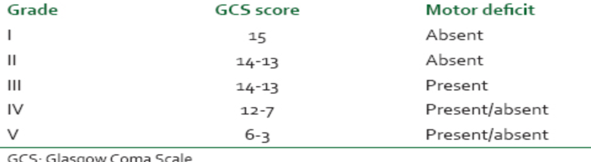
One of the most commonly ones used is the World Federation of Neurologic Surgeons grading system (WFNS). This uses the GCS and the presence or absence of major focal neurologic deficits. Lowest grade is 1. This has the best prognosis.
Once we’ve established the severity of the SAH, the decision is made whether to operate or not. Surgical treatment depends on the condition of the patient, the aneurysm anatomy and the associated vasculature. The options include clipping or endovascular coiling.
Clipping involves placing a clip across the neck of the aneurysm to exclude it from the circulation without occluding any normal vessels. #BBSAH
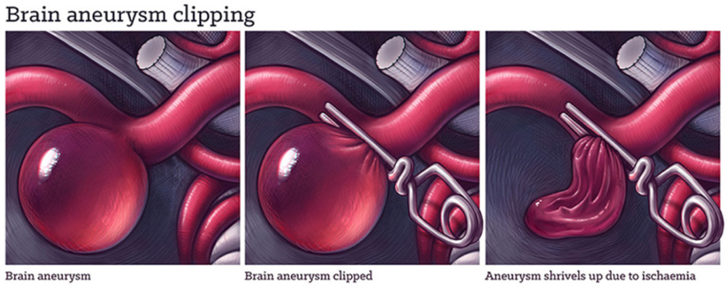
Clipping involves performing a craniotomy to open the skull and enable access to the aneurysm. To understand how we perform a craniotomy here’s one of our video’s showing you how: #BBSAH
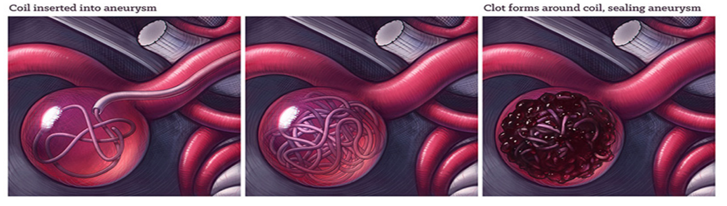
Another option is endovascular coiling. This involves inserting a small tube into an artery in the leg. The tube is advanced up into the artery containing the aneurysm. Coils are then released. This causes clotting of the aneurysm and prevents blood from getting into it. #BBSAH
Our patient was taken to theatre and clipping of her aneurysm was successfully performed. She is now back on the ward and stable. On day 2 you take bloods from the patient and you notice a hyponatremia. She appears dehydrated and is passing large volumes of urine. #BBSAH
What tests need to be performed to work up the hyponatraemia? #BBSAH
You perform a hyponatremia work up which reveals a low serum osmolarity, high urine osmolarity and a high urinary sodium. Does anyone have any thoughts what could be happening? #BBSAH
This is cerebral salt wasting (CSW). CSW can be common after a SAH and is characterised by hyponatremia and fluid depletion due to urinary loss of sodium (remember water follows sodium). This means the patient also appears dehydrated. #BBSAH
So what causes CSW? Well the exact mechanism underlying CSW remains unclear. One theory is that the brain releases brain natriuretic peptide (BNP) after injury. It is thought that this enters the systemic circulation through a disrupted blood-brain barrier. #BBSAH
BNP then acts on the collecting ducts of the renal tubules to inhibit sodium reabsorption as well as decrease the release of renin. #BBSAH
The management of CSW focuses on the correction of the intravascular fluid loss and hyponatremia and the replacement of the urinary sodium loss. For this reason, I.V hypertonic saline is initially prescribed. #BBSAH
It’s very important to ensure that the patient remains hydrated because dehydration can increase the blood viscosity which reduces flow in the blood vessels and can lead to ischemia. #BBSAH
What other complications do we need to consider for our patient? #BBSAH
Answers: Re-bleed, vasospasm, hydrocephalus, seizure. One of the main complications we need to consider is re-bleeding. The consequences of re-bleeding are severe so urgent repair of the ruptured aneurysm by early coiling or surgical clipping is of the utmost importance. #BBSAH
Another complication we need to consider is vasospasm. This occurs because the blood in subarachnoid space is irritant. Inflammatory cytokines are released and this results in smooth muscle contraction in the blood vessel walls and reduces distal blood flow. #BBSAH
Vasospasm can be severe and lead to DNID (Delayed Ischemic Neurological Deficits). So then, how do we prevent vasospasm? #BBSAH
Nimodipine. Nimodipine is a calcium channel blocker which relaxes the smooth muscle walls and causes the vessels to dilate. #BBSAH
Our patient goes into vasospasm. We treat with HHH theraphy (hypervolemia, hypertension and haemodilution). This helps to improve the cerebral blood flow and oxygen delivery to the brain. In refractory cases, intra-arterial nimodipine can also be used. #BBSAH
Our patient is treated with HHH and monitored carefully on the neuro HDU. She remains well post clipping with no neurological deficits. She is discharged after 9 days with a plan to be followed up in clinic. #BBSAH
That's the end of the CBD. We hope this has been useful and you've all learned something.
Your feedback is vital to improve the next CBDs and you'll also get a certificate of participation. We're working towards accreditation ;)
menti.com/cjcy73xmag
It won't take long!
Your feedback is vital to improve the next CBDs and you'll also get a certificate of participation. We're working towards accreditation ;)
menti.com/cjcy73xmag
It won't take long!