@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright They obviously had recruiting problems, given they only found 62 patients with an initial target of 300.
Original plan: (a) control group, (b) 100mg 2x/day, (c) 200mg 2x/day.
100mg 2x/day is underdosed given the IC50. So dropping that group to increase N/group makes sense.
Original plan: (a) control group, (b) 100mg 2x/day, (c) 200mg 2x/day.
100mg 2x/day is underdosed given the IC50. So dropping that group to increase N/group makes sense.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright Not sure re: altered metrics.
I doubt Raoult on prompt viral _clearance_, too much selective omission.
Also, [H]CQ in vitro papers show mechanism is endosome alkalization, which blocks viral entry. Should not directly eliminate free virions, just inhibit further replication.
I doubt Raoult on prompt viral _clearance_, too much selective omission.
Also, [H]CQ in vitro papers show mechanism is endosome alkalization, which blocks viral entry. Should not directly eliminate free virions, just inhibit further replication.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright That implies a few things:
(a) for clearance, patient's immune system must still destroy all accumulated virions and infected cells.
(b) drug should matter more if given early, to mild cases, to prevent further increase in viral load.
(c) clearance may still take a while.
(a) for clearance, patient's immune system must still destroy all accumulated virions and infected cells.
(b) drug should matter more if given early, to mild cases, to prevent further increase in viral load.
(c) clearance may still take a while.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright Consistent with that, a recent French trial found no benefit in N=11 severe cases, and no effect on viral load (which should have indeed been quite high and relatively stable by roughly week 2):
sciencedirect.com/science/articl…
Claiming the drug directly clears the virus makes no sense.
sciencedirect.com/science/articl…
Claiming the drug directly clears the virus makes no sense.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright Most antivirals (this one included) are not 'miracle drugs' -- they are not quick or guaranteed cures.
They mainly just limit further accumulation of viral load, to give the immune system more time to catch up. The immune system is still responsible for cleaning up the mess.
They mainly just limit further accumulation of viral load, to give the immune system more time to catch up. The immune system is still responsible for cleaning up the mess.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright With that in mind:
Time to viral clearance imposes no bound on trial duration. Viral RNA shedding can continue for weeks after recovery:
statnews.com/2020/03/09/peo…
Total clearance is also irrelevant to clinical outcomes. Clearance is plainly not needed for recovery to begin.
Time to viral clearance imposes no bound on trial duration. Viral RNA shedding can continue for weeks after recovery:
statnews.com/2020/03/09/peo…
Total clearance is also irrelevant to clinical outcomes. Clearance is plainly not needed for recovery to begin.
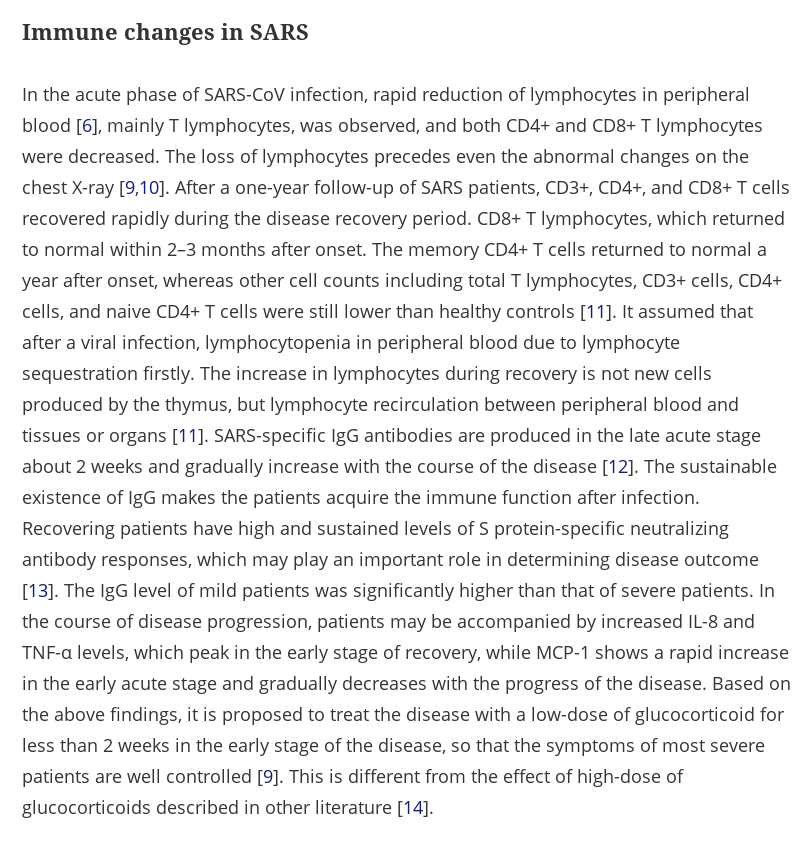
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright As for T cell counts, evidence from SARS suggests it could take months or longer for T cell counts to return to normal (and which subpopulation?), and other leukocyte counts may not fully recover even one year later:
tandfonline.com/doi/full/10.10…
Not a good trial metric, also vague.
tandfonline.com/doi/full/10.10…
Not a good trial metric, also vague.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright I can only speculate on the authors' reasoning, but the original metrics were unsuited to a short-term trial and lack direct clinical relevance.
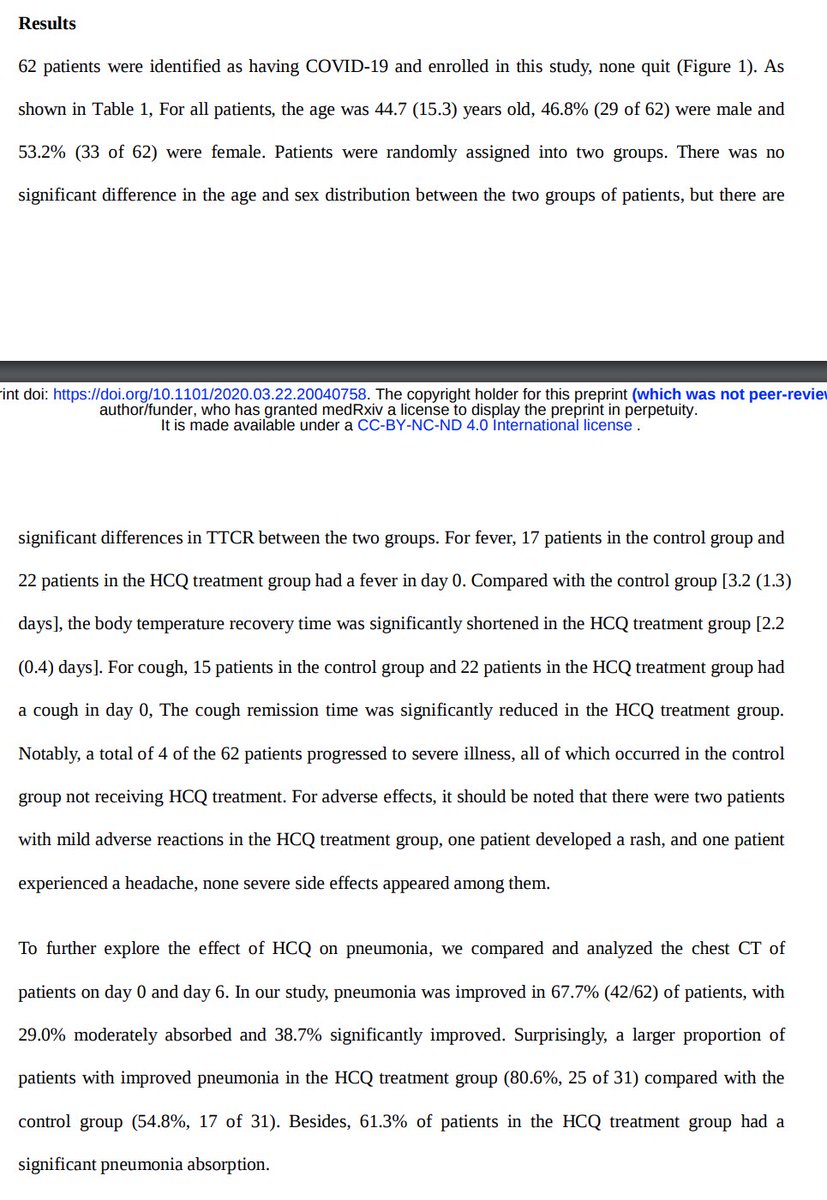
Time to fever and cough reduction, and especially improvement in chest CT, are much more salient to preventing disease progression.
Time to fever and cough reduction, and especially improvement in chest CT, are much more salient to preventing disease progression.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright Hence, regardless of why they chose to make this change (I suspect in order to get their results out sooner), I am glad that they did.
I don't care about time to RNA clearance or leukocyte recovery. That is secondary, and often delayed.
I care about preventing ARDS and death.
I don't care about time to RNA clearance or leukocyte recovery. That is secondary, and often delayed.
I care about preventing ARDS and death.
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright Overall, the results show that the trial succeeded on its clinical metrics:
Fever resolved sooner.
Cough resolved sooner.
Chest CT showed greater improvement in radiological indications of pneumonia.
No progression to severe illness (vs. 13% of controls).
Fever resolved sooner.
Cough resolved sooner.
Chest CT showed greater improvement in radiological indications of pneumonia.
No progression to severe illness (vs. 13% of controls).
@SmutClyde @armand_chatard @schneiderleonid @R_H_Ebright As a *very* interesting side note--
The authors also snuck in a retrospective cohort study of N=80 systemic lupus erythematosis (SLE) patients who used chronic hydroxychloroquine, in Wuhan:
Not a single one had a confirmed case of COVID-19.
Suggests prophylactic value.
The authors also snuck in a retrospective cohort study of N=80 systemic lupus erythematosis (SLE) patients who used chronic hydroxychloroquine, in Wuhan:
Not a single one had a confirmed case of COVID-19.
Suggests prophylactic value.