
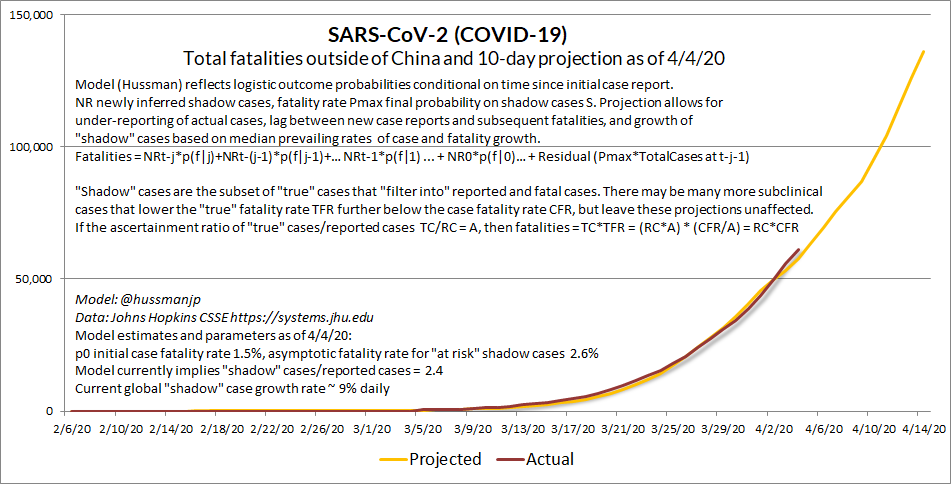
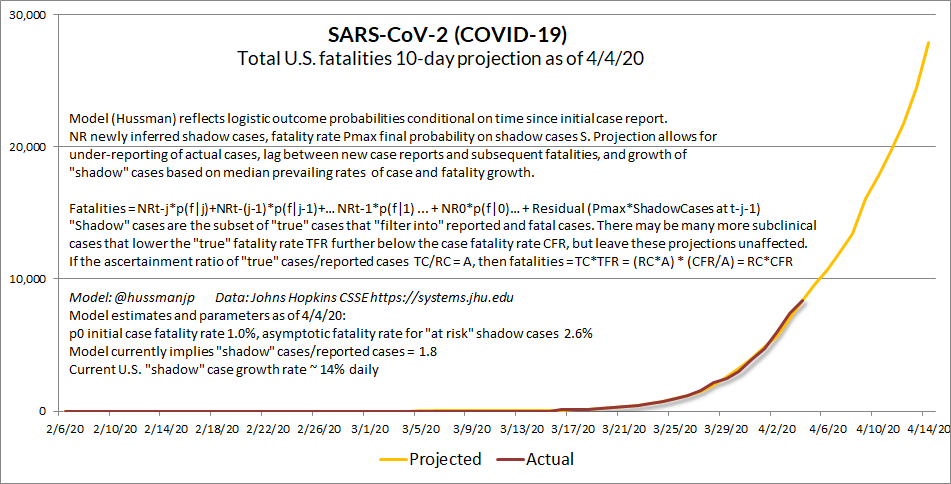
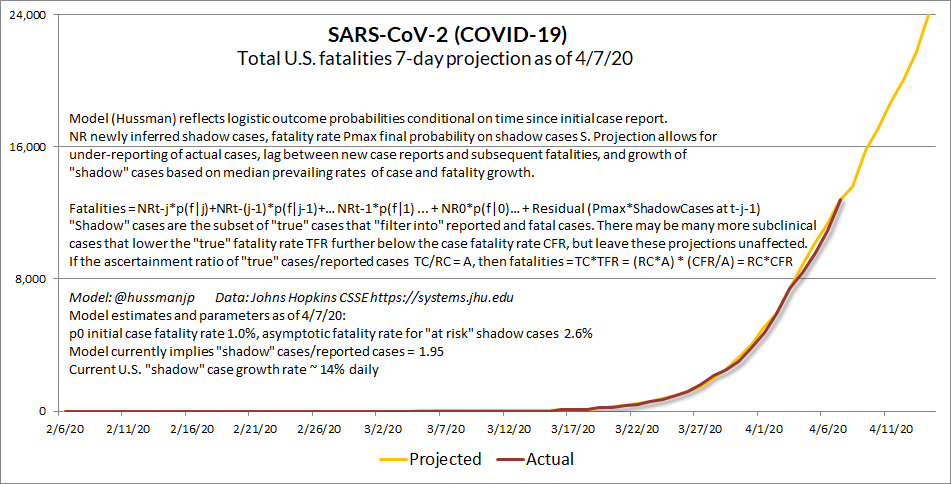
Here's the boostrap projection model I began posting weeks ago, when global fatalities were 12,000, with U.S. 300
Outside U.S., "observed" case fatality rate (CFR) is now above 6%, b/c reported cases are a fraction of total. Fatalities still predictable.

Outside U.S., "observed" case fatality rate (CFR) is now above 6%, b/c reported cases are a fraction of total. Fatalities still predictable.
In the U.S., the notion of 100,000 fatalities "ultimately" or "in the coming months" reflects (my view) incomplete modeling of "shadow" case dynamics, and lag structure between initial case report and fatalities. We risk 100k within weeks without a shift in therapeutic modality.
Snapshot:
a) Weakly contained states, along with mobility, are propagating spread for the entire U.S.
b) Ventilators (high fatality) aren't silver bullets
c) Nor is HCQ, though it may act as DMARD
d) Asking for NIH/NIAID guidance centered on T-lymph inflamm
A friend shared this.
a) Weakly contained states, along with mobility, are propagating spread for the entire U.S.
b) Ventilators (high fatality) aren't silver bullets
c) Nor is HCQ, though it may act as DMARD
d) Asking for NIH/NIAID guidance centered on T-lymph inflamm
A friend shared this.
One way we can gauge the impact of containment is to monitor the projected dates of various catastrophic outcomes (1m U.S. cases, 100k fatalities) using a dynamic model.
Cuomo's early action stopped the future rushing toward us. We're still pushing it back, but not fast enough.
Cuomo's early action stopped the future rushing toward us. We're still pushing it back, but not fast enough.

New (pre-publication) references regarding the IL6 inflammatory axis in #SARSCoV2 (#COVID_19). See my threads for molecular pathway notes.
4/3/20: medrxiv.org/content/10.110…
4/4/20: medrxiv.org/content/10.110…
I'll say it again. We need to shift focus to suppressing the cytokine storm.
4/3/20: medrxiv.org/content/10.110…
4/4/20: medrxiv.org/content/10.110…
I'll say it again. We need to shift focus to suppressing the cytokine storm.

Sharing a notable contraindication for #Hydroxychloroquine in metformin users (JHU). Synergy can result in fatal toxicity. Also note small but important risk of retinal damage more generally. HCQ may be useful, but it's not a magic bullet. See other posts
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
Why interim @NIH / NIAID guidance on repurposed therapeutics urgent for #SARSCoV2 (my views lean to inflammatory T-cell axis - see thread). Among approaches to-date, corticosteroids most common (which literature broadly discourages) & HCQ risks arrhythmia.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
New pre-publications relating to the IL-6/TNF-a axis in #SARSCoV2 / #COVID_19 (all for ICU, not home prophylaxis):
1) medrxiv.org/content/10.110…
2) medrxiv.org/content/10.110…
3) biorxiv.org/content/10.110…
4) medrxiv.org/content/10.110…
5) medrxiv.org/content/10.110…
6) medrxiv.org/content/10.110…
1) medrxiv.org/content/10.110…
2) medrxiv.org/content/10.110…
3) biorxiv.org/content/10.110…
4) medrxiv.org/content/10.110…
5) medrxiv.org/content/10.110…
6) medrxiv.org/content/10.110…



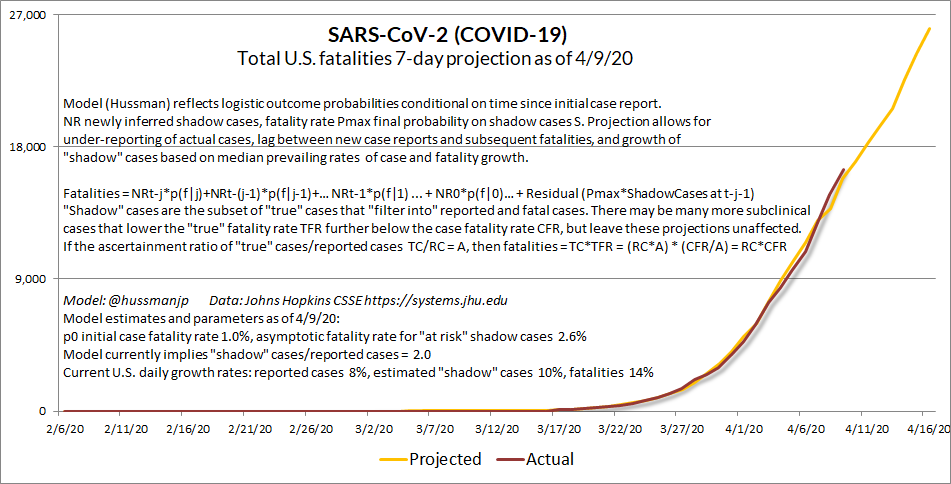
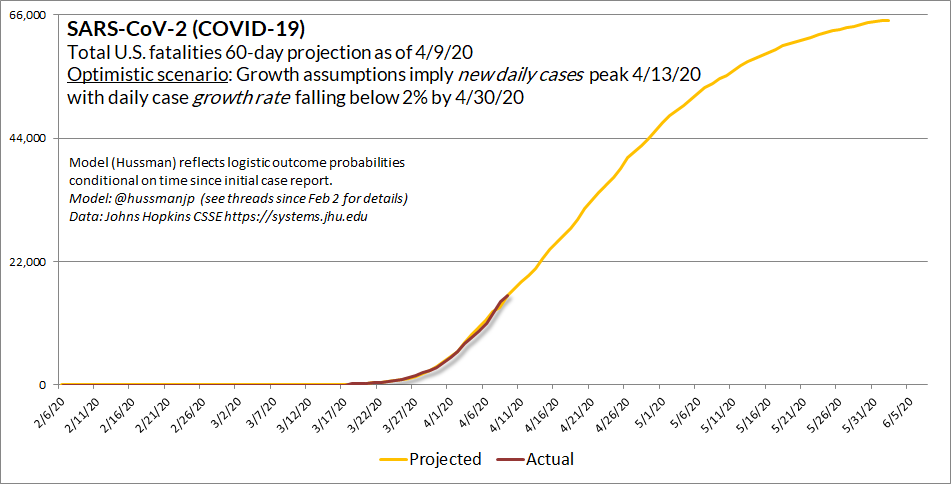
4/9/20 Updated estimate of the plausibly optimistic scenario. Growth rates assume that new daily cases peak on Monday 4/13.
When we talk about "flattening the curve," this is what it might look like. Please don't assume the word "peak" means containment efforts can be relaxed.
When we talk about "flattening the curve," this is what it might look like. Please don't assume the word "peak" means containment efforts can be relaxed.

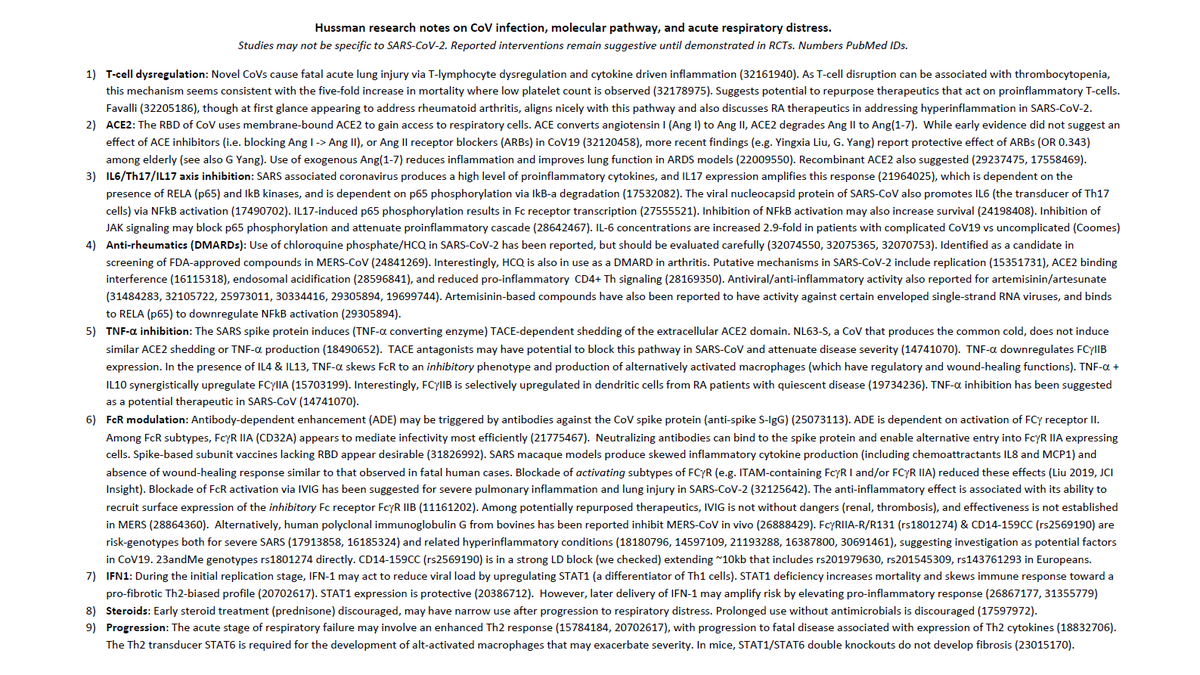
I posted my 4/3/20 #SARSCoV2 (#COVID19) research correspondence to the Foundation website.
Notes on SARS-CoV-2 (COVID-19) inflammatory pathway, and rationale for interim clinical guidance on repurposed therapeutics (possibly on the IL-6/TNF/Th17 axis).
hussmanfoundation.org/articles/SARSC…
Notes on SARS-CoV-2 (COVID-19) inflammatory pathway, and rationale for interim clinical guidance on repurposed therapeutics (possibly on the IL-6/TNF/Th17 axis).
hussmanfoundation.org/articles/SARSC…
Even w/sustained containment efforts, *most U.S. fatalities are likely ahead, unless the therapeutic response in ICUs more directly considers the inflammatory pathway (IL6/TNF-a/Th17/IL17).
My 4/3 memo to research colleagues and NIH/NIAID here. Please RT
hussmanfoundation.org/articles/SARSC…
My 4/3 memo to research colleagues and NIH/NIAID here. Please RT
hussmanfoundation.org/articles/SARSC…

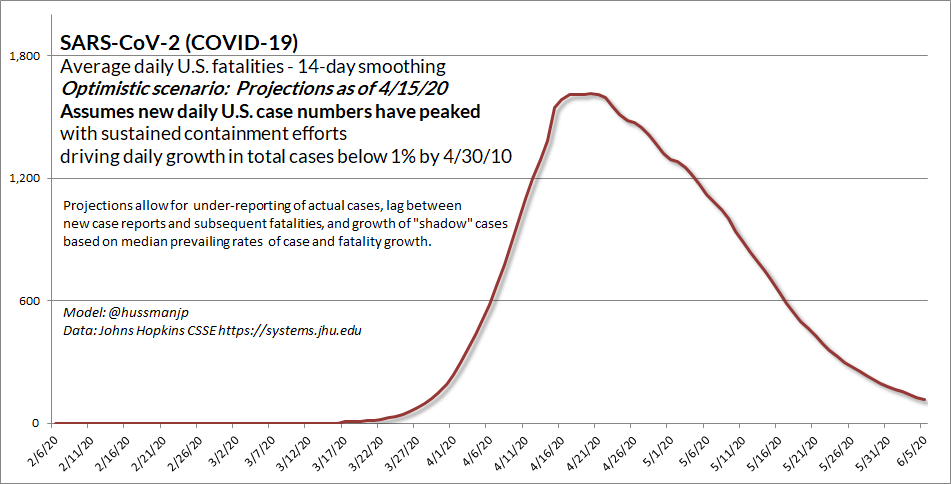
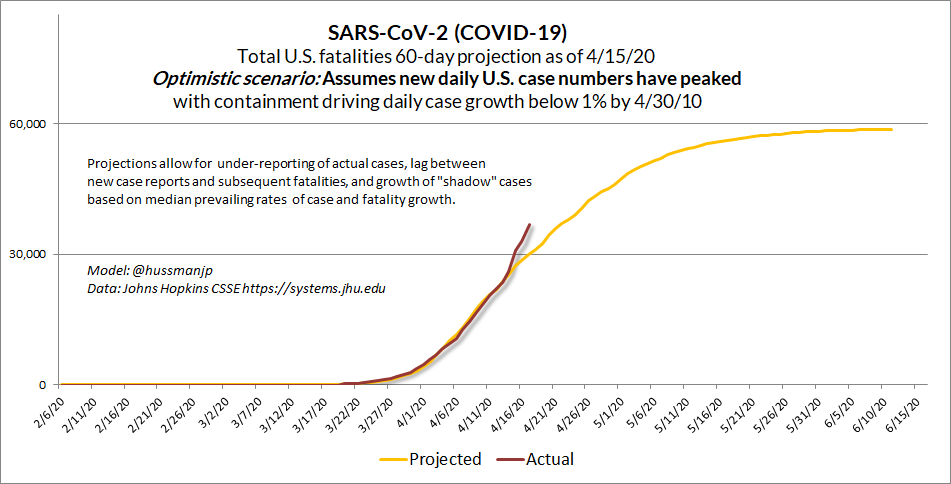
Assuming sustained containment efforts, the "optimistic" projection (my adaptive model) suggests that U.S. daily new cases may have peaked. This does NOT mean these efforts can now be abandoned. Most U.S. fatalities are still ahead, and we still lack capacity to test/track/trace.

Damn. This isn't good. U.S. fatalities just jumped off book. We shouldn't see 31,000 yet.
My hope (if it's possible to hope for such things) is this reflects a lump-sum adjustment for non-ICU fatalities, not a shift in trajectory.
Either way, we have more cases than we thought
My hope (if it's possible to hope for such things) is this reflects a lump-sum adjustment for non-ICU fatalities, not a shift in trajectory.
Either way, we have more cases than we thought

Yes, I think *provided sustained containment efforts (patience...) the number of new daily cases has peaked. My concern, and the reason for patience (for now) is that even in the optimistic scenario, #COVID19 HAS A LONG FAT TAIL. It's not like a storm that's just passed overhead.
Simple, but important. Worth embedding these in the #SARSCoV2 (#COVID_19) thread.
cnn.com/2020/04/14/hea…
cnn.com/2020/04/14/hea…
… thus continuing a crisis response that is nearly indistinguishable from manslaughter.
This is like throwing gasoline on an inferno the very moment firefighters begin to get the blaze under control.
See thread since Feb 2, when we had only 5 cases.
This is like throwing gasoline on an inferno the very moment firefighters begin to get the blaze under control.
See thread since Feb 2, when we had only 5 cases.
A Scottish study similar to Santa Clara sampled donated blood. 4/6 positive cases were drawn from the Edinburgh Health Board area.
They wisely concluded "we cannot use the rise in numbers seropositive to infer the contemporary seropositive or the growth rate of the epidemic."
They wisely concluded "we cannot use the rise in numbers seropositive to infer the contemporary seropositive or the growth rate of the epidemic."
A useful article on designing informed seroprevalence sampling to estimate population infections. With a sample of 3330, the 1.5% prevalence in the Santa Clara study can't exclude zero from its confidence interval. Sample representativeness is an issue.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…






