
#Migraine is the most common & disabling brain disease, but @SocialSecurity still doesn't recognize it as potentially disabling, making it much harder for people to qualify for earned benefits.
🔵Bookmarkable Thread! Info about #SSDI & #disability for migraine.
🔵Bookmarkable Thread! Info about #SSDI & #disability for migraine.
https://twitter.com/JillPiggott/status/1328466468103708673
Globally, #migraine is the #1 cause of disease-related #disability for people 10-24 & the 4th cause for people 25-49. Yet @SocialSecurity still doesn't treat it as a potentially disabling disease. ssa.gov/disability/pro… 

Severe #migraine is profoundly disabling. The World Health Organization uses objective metrics to determine disease burden & ranks severe migraine in the highest category of disability alongside terminal-stage cancer.
Shame on @SocialSecurity.
Shame on @SocialSecurity.

People w/ listed impairments have a 3-step review & must show they're too disabled to do their job. People w/ unlisted impairments have a 5-step review & must show they can't do ANY job even the most sedentary.
#Migraine & severe #headache are unlisted impairments.
#Migraine & severe #headache are unlisted impairments.
People w/ unlisted impairments have to complete the Residual Functional Capacity form (linked).
🟡 The RFC does NOT include Qs about absences, unscheduled breaks, & "time off task": the very things that force people w/ chronic migraine out of work. secure.ssa.gov/apps10/poms/im…
🟡 The RFC does NOT include Qs about absences, unscheduled breaks, & "time off task": the very things that force people w/ chronic migraine out of work. secure.ssa.gov/apps10/poms/im…

#Migraine is unlisted; we apply using epilepsy (11.02) as an analogous listing.
🔵These are the guidelines the person assessing your claim will use to make a determination of migraine disability. Read them & give them to your MD. ssa.gov/OP_Home/ruling…
🔵These are the guidelines the person assessing your claim will use to make a determination of migraine disability. Read them & give them to your MD. ssa.gov/OP_Home/ruling…
Generally, #SocialSecurity considers people unemployable if their doctors anticipate they'll miss 2+ days of work monthly for at least 12 months.
Apply as soon you & your MD think full disability is likely. You can always withdraw your application if you improve.
Apply as soon you & your MD think full disability is likely. You can always withdraw your application if you improve.
I've read 100s of denied appeals as director of @headsUPmigraine. Here are the most common reasons a claim is denied.
#1>Applicant hasn't seen a neurologist, hasn't tried preventive meds, doesn't have a relationship with a doctor, or isn't compliant w/ treatment.
#1>Applicant hasn't seen a neurologist, hasn't tried preventive meds, doesn't have a relationship with a doctor, or isn't compliant w/ treatment.
I've read multiple files where judges agree the applicant has chronic migraine, but deny benefits because the person is only using OTC pain med (Excedrin Migraine!) &/or occasionally going to the ER.
‼️ PLEASE don't try to to manage a progressive brain disease over the counter.
‼️ PLEASE don't try to to manage a progressive brain disease over the counter.
If med doesn't help or you can't afford it, say so. If you live far from a neurologist, ask your PCP to team up with a specialist, so you can consult with the specialist every 12-18 months but follow up regularly with your PCP.
#2>Applicant doesn't identify anything she's done to stay employed despite increasing disability.
This can include anything from asking to work in an area w/o no fluorescents to changing jobs hoping to find work that fits your decreased level of function.
This can include anything from asking to work in an area w/o no fluorescents to changing jobs hoping to find work that fits your decreased level of function.
Remember: people w/ listed impairments only have to show they can no longer do their jobs. #Migraine is unlisted. We have to show we can't do ANY job.
#SocialSecurity thinks there are jobs suitable for sedentary CLAMS & therefore suitable for migraineurs.
#SocialSecurity thinks there are jobs suitable for sedentary CLAMS & therefore suitable for migraineurs.
#3>Applicant hasn't anticipated Social Security's "solution" (find a sedentary job) & thus hasn't shown she can't do ANY job because she's often absent or arrives late, takes unscheduled breaks, leaves early, or functions below 50% productivity.
🔵This is your whole case!
🔵This is your whole case!
Quantify your disability w/ official records of missed work or school. Ask a coworker for a letter if you can't get a boss or HR to help. Keep records like a #migraine diary or a chart of missed activities & obligations. Share these with your MD.
#4>The applicant hasn't specified how her symptoms reduce her function.
SSA & insurers don't care about how we FEEL; they care about what we can DO. Not "I hurt all the time," but "Pain-related fatigue means for every 1/2 hour I'm up, I spend 2 hours lying down."
SSA & insurers don't care about how we FEEL; they care about what we can DO. Not "I hurt all the time," but "Pain-related fatigue means for every 1/2 hour I'm up, I spend 2 hours lying down."
"I'm dizzy a lot"="At least 2 days a week, I'm so dizzy, I can't even do small things like unload the dishwasher."
"Light really bothers me"="It's no longer safe for me to drive because flickering light in the day & headlights at night make me disoriented & nauseous."
"Light really bothers me"="It's no longer safe for me to drive because flickering light in the day & headlights at night make me disoriented & nauseous."
Unjustly denied claims make me mad.
1. Some judges generalize sentences in patient records like "Patient says she's doing better." I hope avoiding mistakes 1-6 will help protect you from this.
1. Some judges generalize sentences in patient records like "Patient says she's doing better." I hope avoiding mistakes 1-6 will help protect you from this.
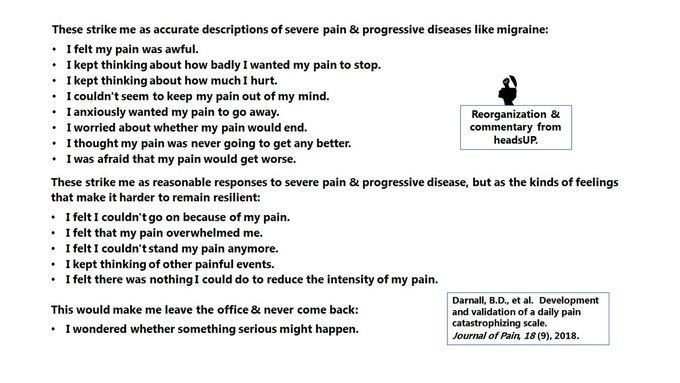
2) Sometimes judges base denials on psych tests or diagnoses of "catastrophizing, rumination, &/or magnification." A judge hung an entire denial on this sentence earlier in 2020: "He described a number of maladaptive thoughts & beliefs about pain (Pain Catastrophizing Scale)."
The "catastrophizing" survey asks how often you have specific thoughts or feelings about pain (see pic). headsUP thinks it overdiagnoses anxiety.
🔴Be aware that judges sometimes use the test when assessing disability claims. You can always decline to take it.
🔴Be aware that judges sometimes use the test when assessing disability claims. You can always decline to take it.
Other tips: SSA often uses 2 terms when describing successful migraine claims: "lying down" & "dark, quiet place." Most workplace don't have a dark, quiet place where you can lie down. Use the terms to describe #FullZonk even if it hurts to lie flat & your place is never quiet.
#Migraine is a highly variable disease. When I 1st started reading about it, I was surprised to realize that I didn't have a lot of different things "wrong" with me. I had migraine. Understanding its range can help you better explain how it disables you.

Post any questions you have in the @headsUPmigraine (no-rule!) public facebook group. Lots of us have been through the disability application process, & someone's sure to have good advice. Bring jokes. facebook.com/groups/6382986…
The book "Nolo's Guide to Social Security Disability: Getting & Keeping Your Benefits" is a good general intro & probably available in your local library. NOLO's website is also useful. nolo.com/legal-encyclop…
See also National Disability Forum: Developing and Assessing Medical Evidence for Extreme Limitations in the Ability to Focus on Tasks posted by #SocialSecurity. ssa.gov/ndf/documents/…
@threadreaderapp unroll
@NitaGhei
@threadreaderapp unroll
@NitaGhei
• • •
Missing some Tweet in this thread? You can try to
force a refresh




