1/ Estimating the infection fatality risk (IFR) of #SARSCoV2 is hard.
Our estimates from Spain's #ENECOVID (just published):
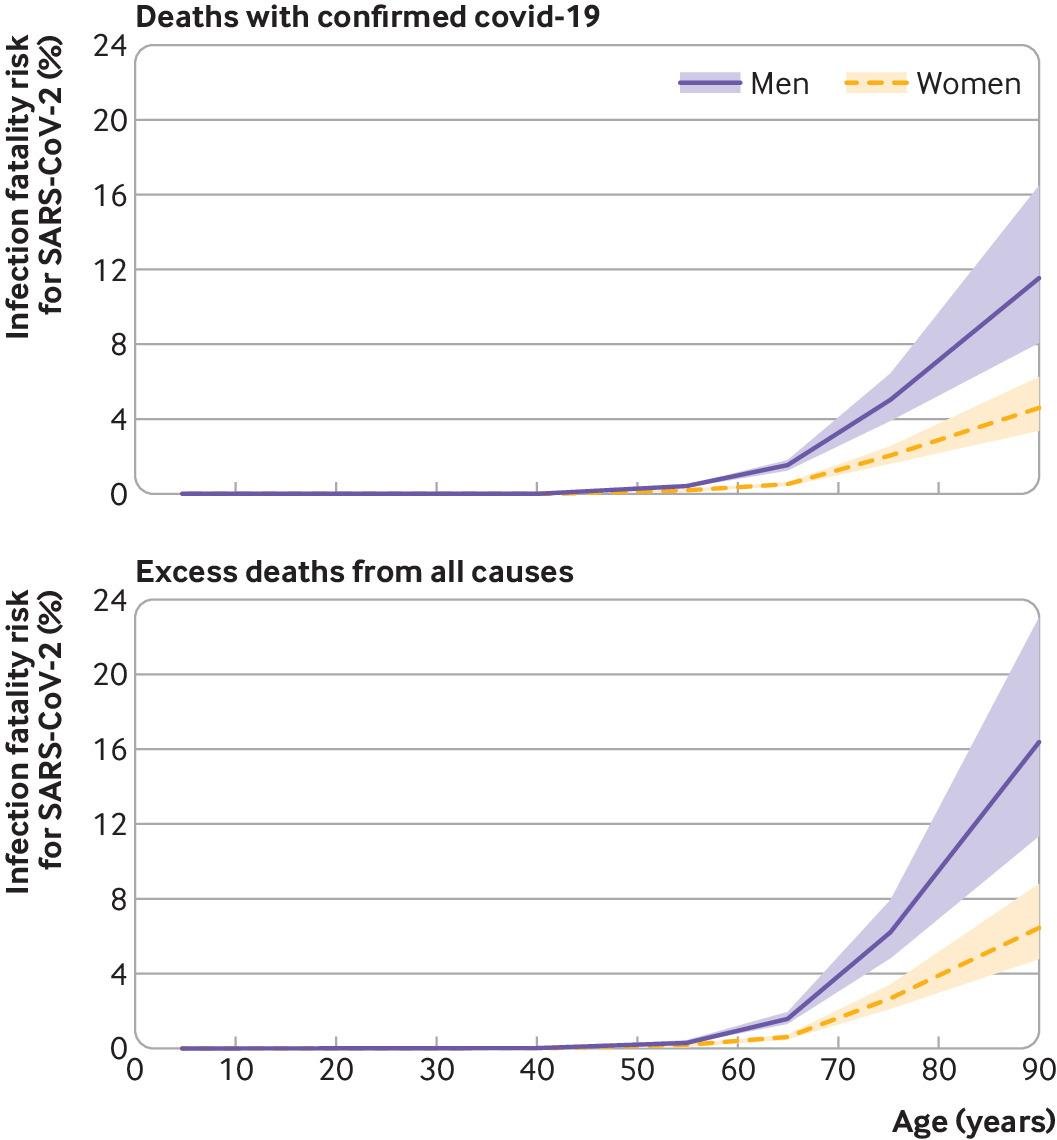
Men: 1.1% to 1.4%
Women: 0.58% to 0.77%
After age 80
Men: 12% to 16%
Women: 4.6% to 6.5%
Why is the #IFR hard to estimate?
bmj.com/content/371/bm…
Our estimates from Spain's #ENECOVID (just published):
Men: 1.1% to 1.4%
Women: 0.58% to 0.77%
After age 80
Men: 12% to 16%
Women: 4.6% to 6.5%
Why is the #IFR hard to estimate?
bmj.com/content/371/bm…
2/ The IFR in a population is the ratio of
number of deaths from SARS-CoV-2 infection (numerator)
and
number of individuals infected by SARS-CoV-2 (denominator)
during a prespecified period.
Both numerator and denominator are hard to quantify.
number of deaths from SARS-CoV-2 infection (numerator)
and
number of individuals infected by SARS-CoV-2 (denominator)
during a prespecified period.
Both numerator and denominator are hard to quantify.
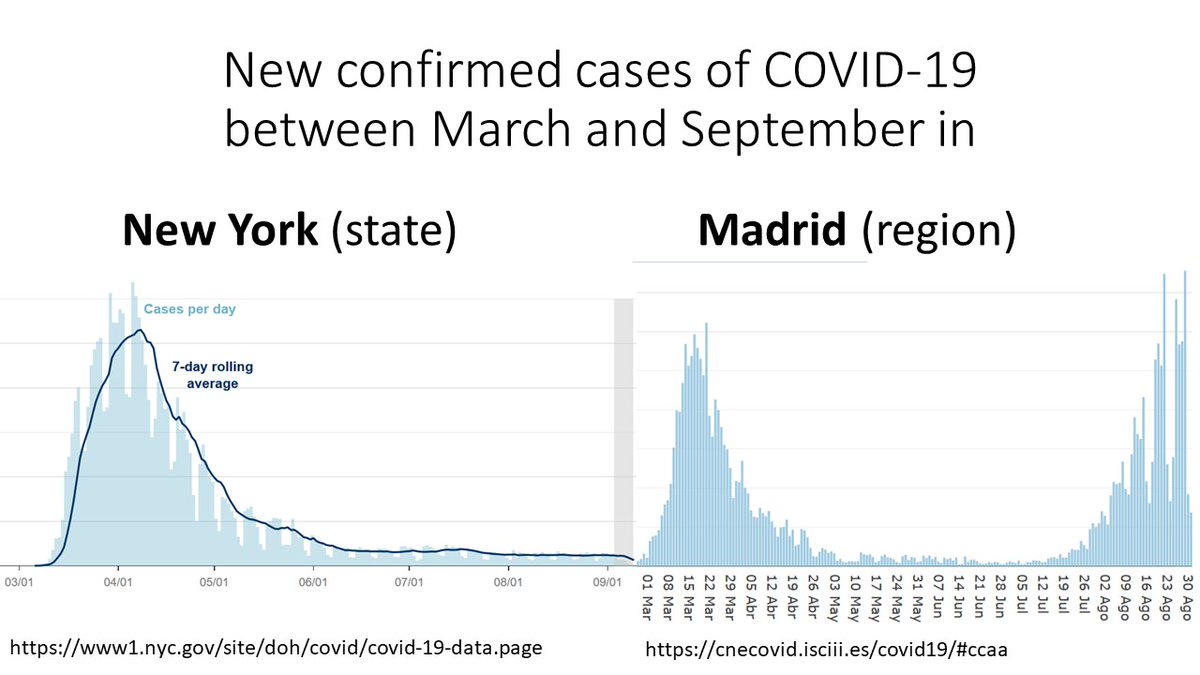
3/ Why is the denominator hard to quantify?
The number of infected with #SARSCoV2 is not the number of confirmed #COVID19 cases.
Because many infected individuals never have symptoms or have minor symptoms and are never diagnosed.
(For details, see journals.plos.org/plosntds/artic…)
The number of infected with #SARSCoV2 is not the number of confirmed #COVID19 cases.
Because many infected individuals never have symptoms or have minor symptoms and are never diagnosed.
(For details, see journals.plos.org/plosntds/artic…)
4/ Need to identify the infected via a serosurvey:
Measure antibodies against #SARSCoV2 in a large, random sample and extrapolate to the entire population.
Make sure serosurvey happens before people lose antibodies.
That's how #ENECOVID was designed.
thelancet.com/journals/lance…
Measure antibodies against #SARSCoV2 in a large, random sample and extrapolate to the entire population.
Make sure serosurvey happens before people lose antibodies.
That's how #ENECOVID was designed.
thelancet.com/journals/lance…
5/ Why is the numerator hard to quantify?
The number of deaths may be
underestimated by confirmed #COVID19 deaths because of incomplete ascertainment.
overestimated by excess deaths because of indirect effects of the pandemic.
We used both numbers and provided the range.
The number of deaths may be
underestimated by confirmed #COVID19 deaths because of incomplete ascertainment.
overestimated by excess deaths because of indirect effects of the pandemic.
We used both numbers and provided the range.
6/ Thanks to everyone who make #ENECOVID possible
@SaludISCIII, @sanidadgob, and regional Health Departments.
Over 60,000 participants
4400 health professionals
1409 health care centers
29 laboratories
throughout the Spanish National Health System.
Next round is ongoing.
@SaludISCIII, @sanidadgob, and regional Health Departments.
Over 60,000 participants
4400 health professionals
1409 health care centers
29 laboratories
throughout the Spanish National Health System.
Next round is ongoing.
• • •
Missing some Tweet in this thread? You can try to
force a refresh