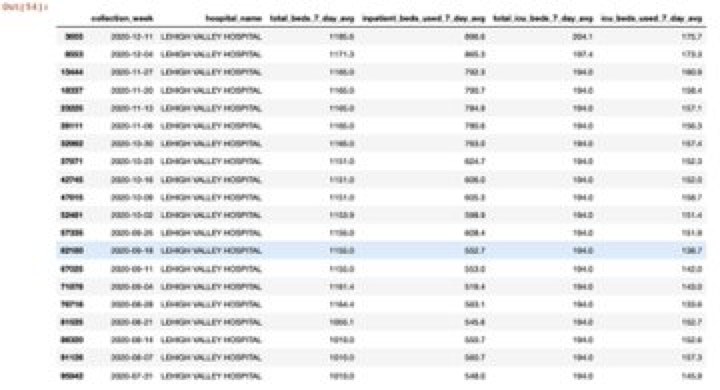
#Healthcare is just an interesting business to be a part of. I saw a fellow post details from the PSU Health website that included a bunch of information in json format. I was curious to see what the data revealed. 1/n 

2/n The most interesting surprise, aside from specific breakdowns of variation in reimbursement per service by payer, was the specific classification for "Amish/Mennonite OP Rate".



@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh