Why are numbers in Kerala an anomaly ?
Here is my take on these numbers
Here is my take on these numbers
https://twitter.com/NewsBytesApp/status/1412738394547908610
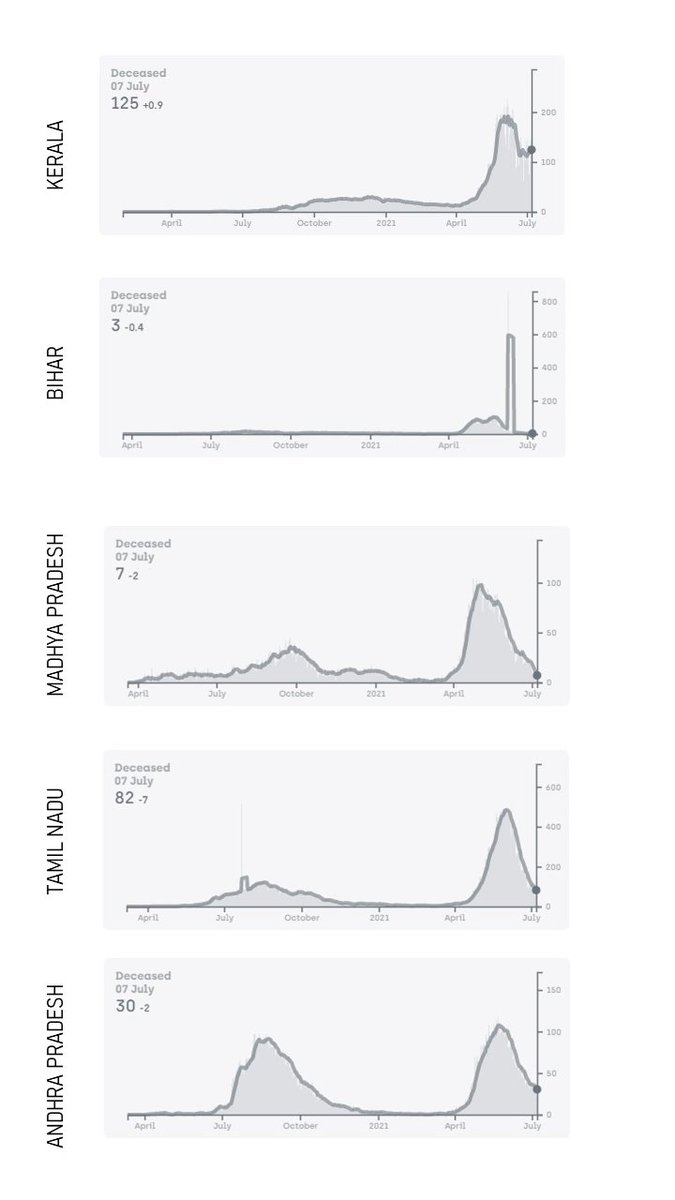
No. of cases are not directly comparable across states, due to the large disparity in testing capacities. It is most likely that the high nos are just representative of the testing nos. Here is a comparison of some states. Data from covid19india.org 

So are the COVID-19 deaths for the states. Of note and contrast would be Kerala and Bihar - see closely the no of tests and deaths
There are also concerns on veracity of these nos theprint.in/opinion/benfor…
Therefore people have used an indirect measure called "excess deaths". The basic assumption is that any "excess" compared to previous year estimates could be suggestive of "missing" COVID-19 deaths
Therefore people have used an indirect measure called "excess deaths". The basic assumption is that any "excess" compared to previous year estimates could be suggestive of "missing" COVID-19 deaths
@Rukmini has a wonderful compilation of the "excess deaths" for these states
https://twitter.com/Rukmini/status/1412287526941900803?s=20
Therefore what we need to compare is whether the case nos could be effectively managed.
There is now evidence to suggest overloading hospitals could significantly contribute to the mortality rates nature.com/articles/s4146…
There is now evidence to suggest overloading hospitals could significantly contribute to the mortality rates nature.com/articles/s4146…
The need of the day is therefore to discuss on how to create public health systems to appropriately identify (test) and manage cases and get early warning from systematic genomic surveillance , rather than comparisons of uncomparable numbers.
The full article is here scroll.in/article/998620… @Rukmini
• • •
Missing some Tweet in this thread? You can try to
force a refresh