
1) Welcome to a new #accredited #tweetorial, Prevention and Management of Heart Failure in T2 Diabetes: The Cardiologist’s Perspective! Our expert author is Giuseppe Galati MD, MMSc in Heart Failure, @GiuseppeGalati_ , Consultant #Cardiologist #HeartFailure & #Cardiomyopathies 

2) @GiuseppeGalati_ is at San Raffaele Research Hospital, Milan 🇮🇹 @SanRaffaeleMI. This program is intended for #healthcare professionals & is accredited for 0.75h CE/#CME credit for #physicians #physicianassistants #nurses #nursepractitioners #pharmacists 🇺🇸🇨🇦🇬🇧🇪🇺.
3) @cardiomet_CE is supported by educational grants from AstraZeneca, Bayer, Boehringer Ingelheim Pharmaceuticals Inc. and Eli Lilly Company, & Chiesi. Earn credit from archived programs at cardiometabolic-ce.com. Disclosures at cardiometabolic-ce.com/disclosures/.🙏 FOLLOW US !
4) #DiabetesMellitus (#T2DM) is highly prevalent in #HeartFailure patients. In this US registry of patients hospitalized for #AcuteHF the prevalence of #T2DM has been remained constant from 2005 to 2015: 40-45% both in #HFrEF & #HFpEF
See 🔓pubmed.ncbi.nlm.nih.gov/32486833/
See 🔓pubmed.ncbi.nlm.nih.gov/32486833/

5) The presence of #T2DM is associated with increased all-cause mortality in #HF without significant differences between #HFrEF & #HFpEF.
See 🔓pubmed.ncbi.nlm.nih.gov/32486833/
See 🔓pubmed.ncbi.nlm.nih.gov/32486833/

6) In this Italian cohort 🇮🇹 the prevalence of #T2DM showed to be high, not only in hospitalized patients, but also in #chronicHF. It was nearly 35% both in #HFrEF & in #HFpEF.
See 🔓pubmed.ncbi.nlm.nih.gov/29917301/
See 🔓pubmed.ncbi.nlm.nih.gov/29917301/

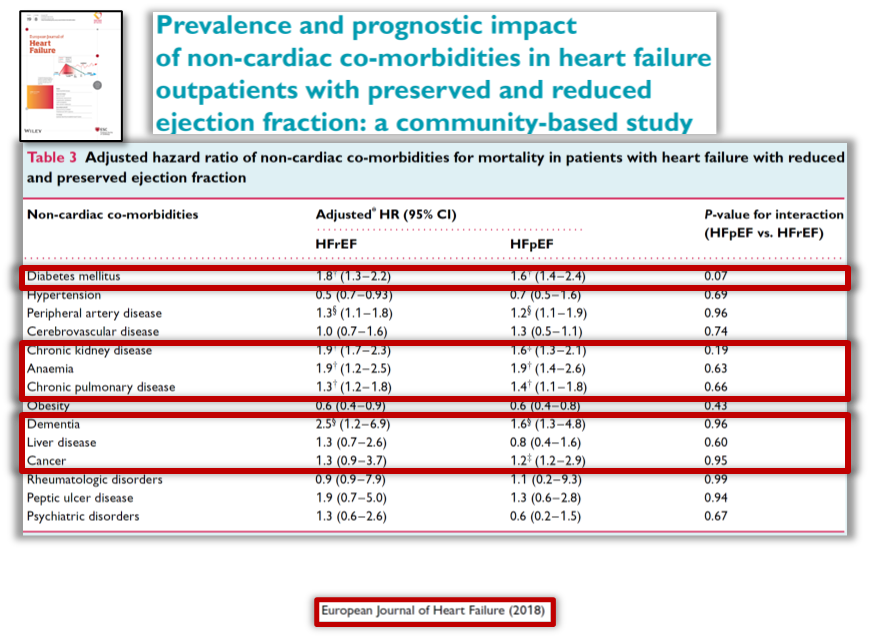
7) #TD2M showed to be one of the most important comorbidities in #HF as a multiplier of the risk of mortality in these patients, across the full spectrum of #LVEF
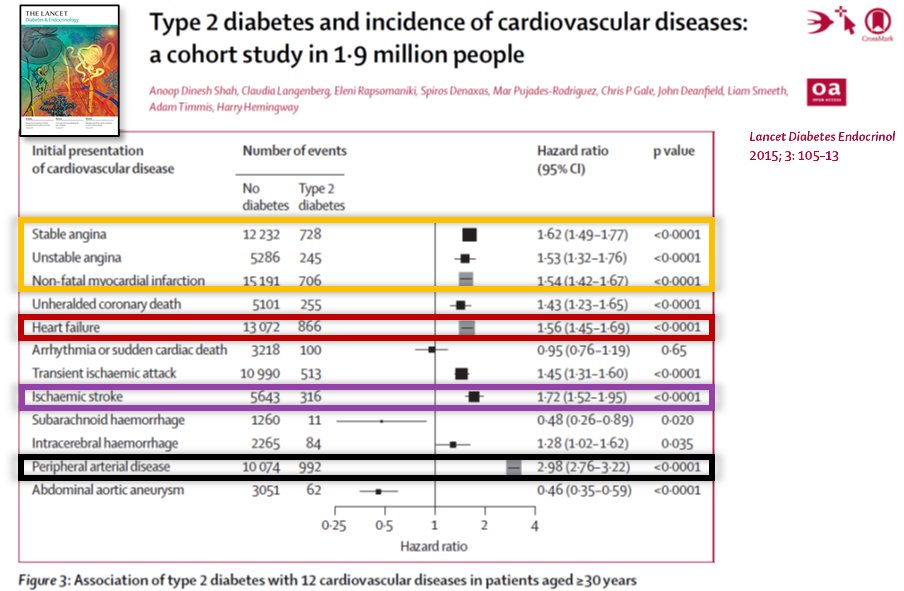
8) Diabetic patients have a higher risk not only of #AcuteCoronarySindrome but also of #HF, #IschemicStroke and #PeripheralArteryDisease. Despite it is poorly known, the risk of developing #HF is comparable to that of having an #ACS.
See 🔓pubmed.ncbi.nlm.nih.gov/25466521/
See 🔓pubmed.ncbi.nlm.nih.gov/25466521/
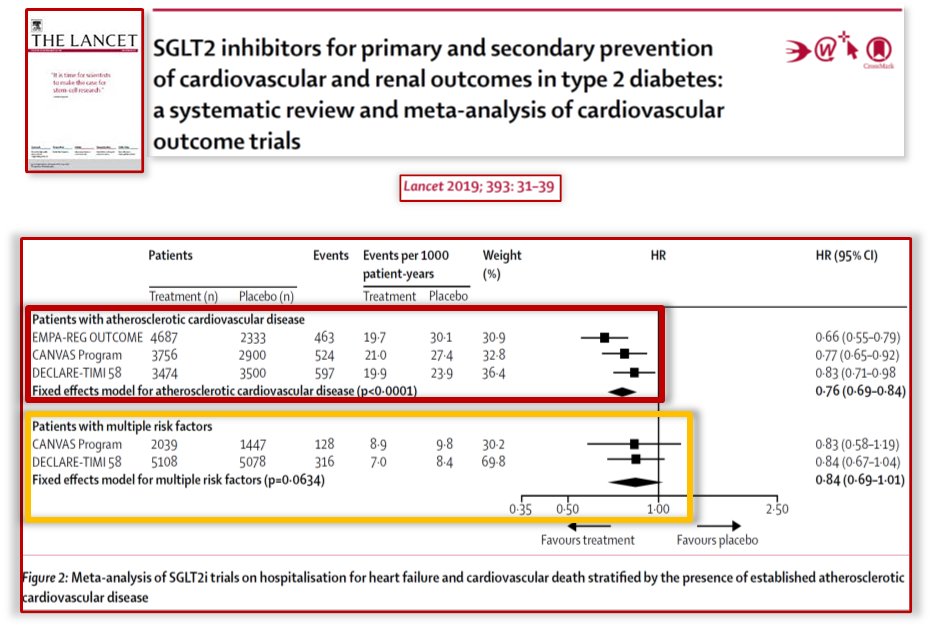
9) Sodium-Glucose type2 inhibitors #SGLT2i in large trials for prevention in #T2DM pts showed significant ⬇️risk of #MACE (major #cardiovascular events) & #CV_Death in pts with atherosclerotic #CV disease, with a positive trend in pts without #ASCVD
See pubmed.ncbi.nlm.nih.gov/30424892/
See pubmed.ncbi.nlm.nih.gov/30424892/
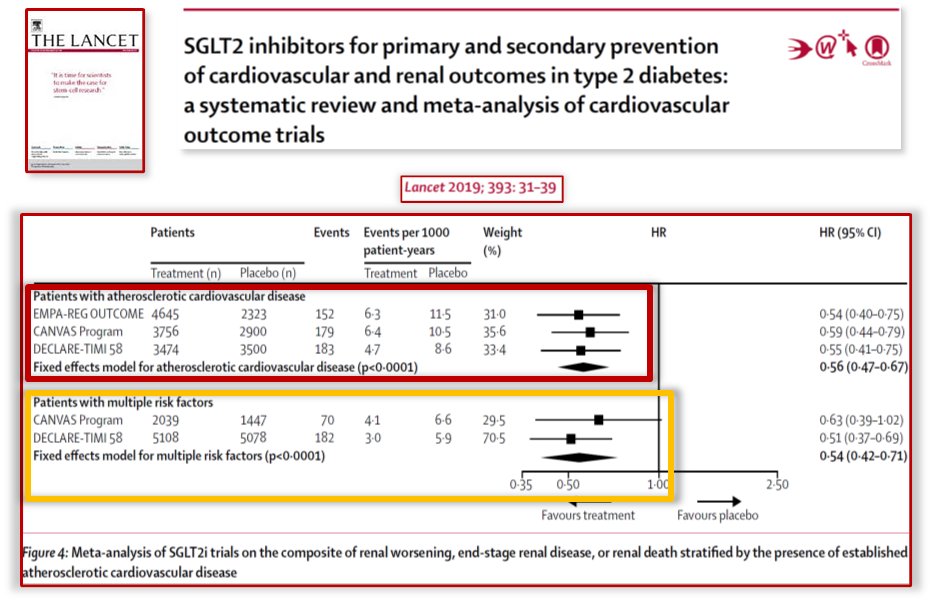
10) However, the major driver of benefit in these trials dedicated to prevention has been the reduction of #HF hospitalizations #HHF & #CV_Death. The developers of these drugs thus decided to test them in #RCT dedicated to #HF +/- #T2DM status.
See pubmed.ncbi.nlm.nih.gov/30424892/
See pubmed.ncbi.nlm.nih.gov/30424892/
11) The 1st #RCT published in #HFrEF patients was #DAPA_HF. This trial enrolled >4700 #HFrEF pts irrespective of #T2DM status (see inclusion criteria). Primary EP was combined #CV_Death, #HHF & #UrgentHFvisit. Mean follow-up has been 18.2 months.
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/
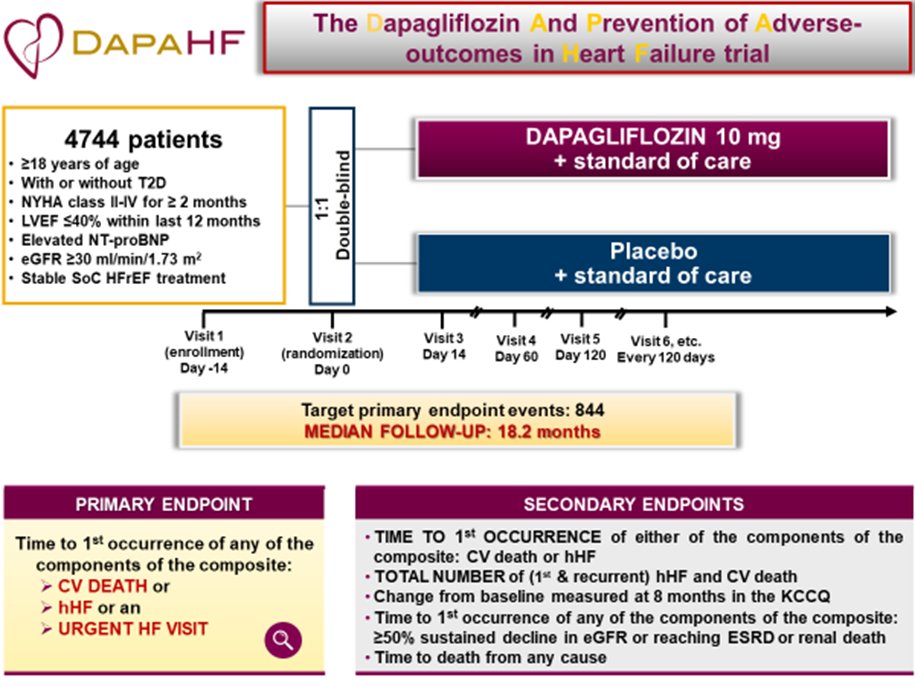
12) Here you can see the characteristics of the enrolled population. 67% of NYHA II, mean #LVEF: 31%, median #NT-proBNP: 1400 pg/mL, Previous #HHF 47%, #TDM 42%, mean #eGFR 65 ml/min.
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/

13a) #DAPA_HF was the first #RCT that demonstrated that an #SGLT2i significantly reduced the primary EP (#CV_Death + 1st #HHF + #UrgentVisitForH) in #HFrEF patients irrespective of #T2DM status with an RRR of 26%.
13b) The pre-specified primary #EP analysis showed that the benefit was significant and with the same magnitude both in diabetic vs non-diabetic pts.
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/

14) One year later #EMPEROR_REDUCED was published. This trial enrolled >3700 #HFrEF patients irrespective of #TD2M status with a similar design of #DAPA_HF. The mean follow-up was shorter than DAPA_HF i.e. 16 months.
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/
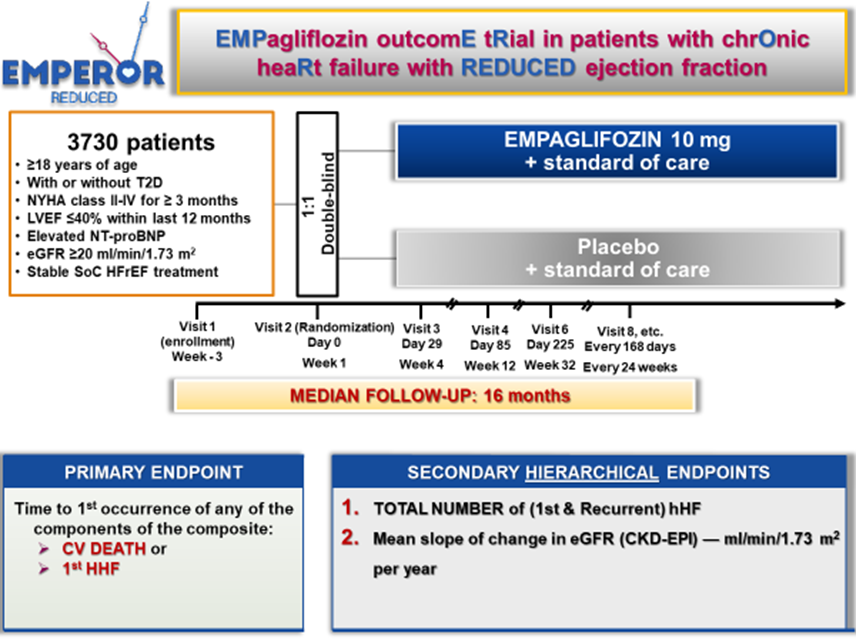
15) The population enrolled in #EMPEROR_REDUCED when compared to that of #DAPA_HF had higher NYHA III 24% , lower mean #LVEF: 27%, and higher #NT_proBNP level: 1900 pg/mL. Previous #HHF 31%, #TDM 50%, mean #eGFR 62 ml/min
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/
See 🔓pubmed.ncbi.nlm.nih.gov/31535829/

16) A head-to-head comparison of #DAPA_HF vs #EMPEROR_REDUCED showed that #EMPEROR_REDUCED enrolled a more severe #HFrEF population, providing complimentary data of efficacy and safety in #HFrEF when compared to DAPA_HF.

17) As in #DAPA_HF, #EMPEROR_REDUCED showed significant ⬇️in the primary #EP (#CV_Death + 1st #HHF) in #HFrEF patients irrespective of #T2DM status; RRR 25%. Pre-specified primary #EP analysis ➡️benefit was significant & with similar magnitude in diabetic vs non-diabetic pts.

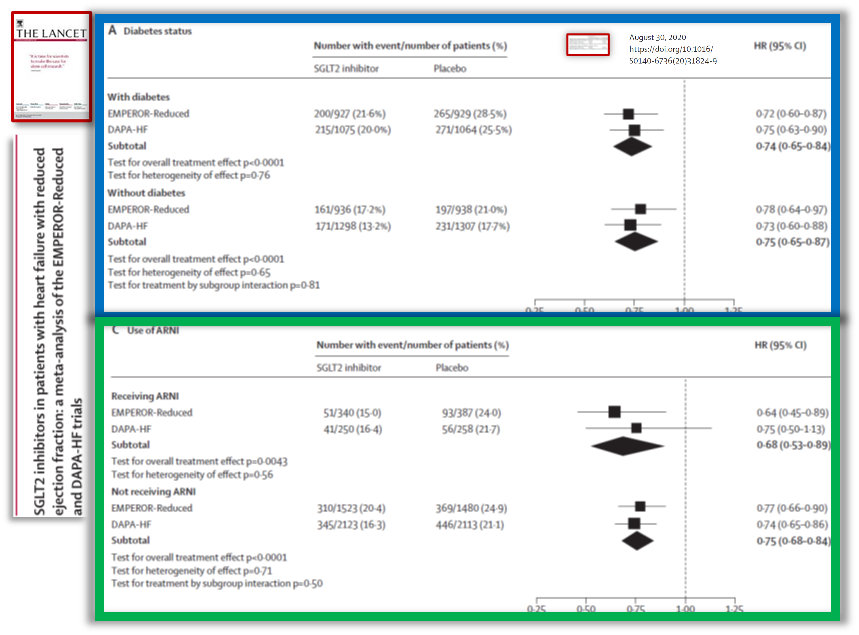
18) The first metanalysis published in Lancet in 2020 showed without any doubt that #SGLT2i in #HFrEF pts significantly reduced: #CV_Death + 1st #HHF, & #CV_death & ALL-Cause Death when considered alone.
See pubmed.ncbi.nlm.nih.gov/32877652/
See pubmed.ncbi.nlm.nih.gov/32877652/

19) This metanalysis showed that SGLT2i significantly reduced 1st #HHF when considered alone, Total (1st + recurrent) #HHF + #CV_Death & significantly reduced renal outcomes.
The benefit on renal outcomes confirmed what was demonstrated in RCTs dedicated to prevention in #T2DM
The benefit on renal outcomes confirmed what was demonstrated in RCTs dedicated to prevention in #T2DM

20) The benefit of SGLT2i in #HFrEF on primary EP (#CV_Death + 1st #HHF) was independent of diabetes status and of #ARNI therapy, i.e. it was the same in patients with or without diabetes, receiving or not ARNI.
See pubmed.ncbi.nlm.nih.gov/32877652/
See pubmed.ncbi.nlm.nih.gov/32877652/
21) The same benefit of #SGLT2i in #HFrEF on primary EP was independent of #eGFR.
In particular the benefit was the same in patient with eGFR > or < than 60 ml/min.
In particular the benefit was the same in patient with eGFR > or < than 60 ml/min.

22a) So what have you learned? #SGLT2i therapy has been shown to improve outcomes in #CVOTs except for which ONE of the following?
22b) Enter your response & return TOMORROW for the correct answer & the remainder of this #accredited #tweetorial! 👍to @GoggleDocs @DrMarthaGulati @mmamas1973 @SABOURETCardio @HanCardiomd @SeguraCardio @ValleAlfonso @gcfmd @purviparwani @DFCapodanno @mirvatalasnag @gbiondizoccai
23) Welcome back! We are reviewing the #cardiology perspective on the #prevention & #management of #HF in pts with #T2D. I am @GiuseppeGalati_ & I encourage you to follow @cardiomet_CE for all your #cardiometabolic CE/#CME needs! 👏to @ShivangiPraman1 @bianchinifra92 @edurontoFF
24) Yesterday's knowledge ✔️? Scroll back up to 22a) and answer if you didn't already! The answer is c. In pts with #diabetes, #SGLT2i's ⬆️risk of #hyperkalemia in those w/stage 3 or higher #CKD vs those with stage 1, 2, or no CKD. Even #flozins can't do EVERYTHING!
25) After demonstrating sig benefit in #T2DM & #chronic #HFrEF, #SGLT2i was evaluated in a pilot trial dedicated to #acute #HF #AHF. #EMPA_RESPONSE_AHF enrolled 80 patients hospitalized for #AHF & significantly⬆️diuretic response on top of furosemide.
See🔓pubmed.ncbi.nlm.nih.gov/31912605
See🔓pubmed.ncbi.nlm.nih.gov/31912605

26) #EMPA_RESPONSE_AHF (🔓pubmed.ncbi.nlm.nih.gov/31912605/) showed encouraging results on reduction of #HHF, Worsening #HF and #Death. Clearly, due to the very small sample size this has been just a hypothesis-generator. But this RCT started a new path of #SGLT2i in #AHF


27) The first large RCT dedicated to #SGLT2i + #SGLT1i in #AHF was #SOLOIST_WHF. This #RCT dedicated to #TD2M + #AHF pts enrolled >1200 pts. Here you can see the design of this RCT, led by @CardioMet faculty @DLBHATTMD
🔓pubmed.ncbi.nlm.nih.gov/33200892/
🔓pubmed.ncbi.nlm.nih.gov/33200892/

28) #SOLOIST_WHF enrolled #TD2M + #AHF pts, with the following characteristics: included all the spectrum of #LVEF (HFrEF, HFmrEF, HFpEF) and all the #NYHA classes (majority II & III), median #NT-proBNP: 1800 pg/mL

29) #SOLOIST_WHF was the first RCT that demonstrated in pts with #AHF + #T2DM a significant ⬇️of the Primary #EP: #Total #CV_death + #HHF + #UrgentVisitForHF, but due to change of the Primary EP because of the #Covid19 & change in sponsorship a further proof was needed

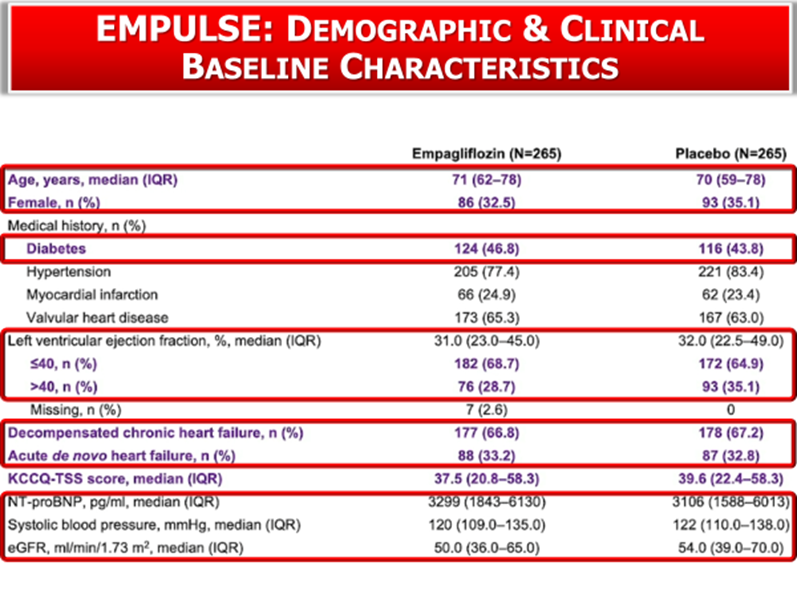
30) #EMPULSE, presented at last #AHA21, was the first large RCT dedicated to #SGLT2i in #AHF irrespective of #T2DM status. Here you can see the trial design: any #LVEF, high level of #NT-proBNP_BNP, randomization between 24h and 5d after #HHF
See 🔓pubmed.ncbi.nlm.nih.gov/35228754/
See 🔓pubmed.ncbi.nlm.nih.gov/35228754/

31) #EMPULSE enrolled 530 #AHF pts with these characteristics: #T2DM 45%, median #LVEF: 31%; #HFrEF 66%, #HFmrEF + #HFpEF 33%, median #NTproBNP: 3180 pg/mL, median eGFR 52%, de-novo #AHF 33%, worsening #AHF/ decompensated #CHF 66<%
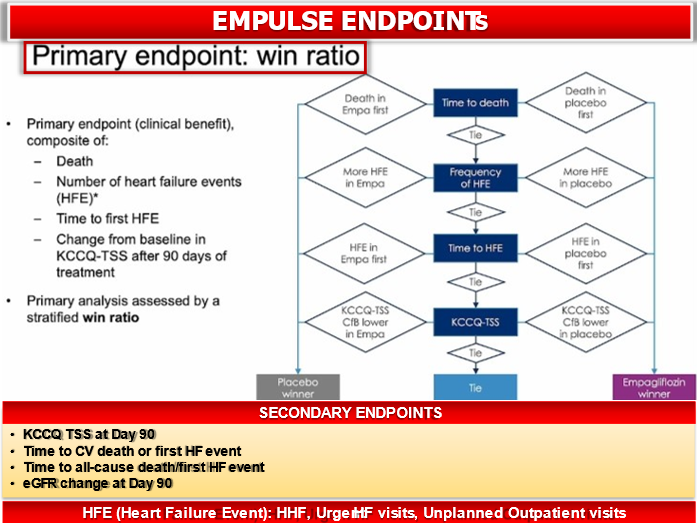
32) #EMPULSE reduced the Primary #EP a composite of: #All_cause_Death, #HFEvent frequency, #Time to first #HFE, #KCCQ_TTS. This was the first RCT in the history of #cardiology to achieve this in #AHF independently from diabetes status. 🔓pubmed.ncbi.nlm.nih.gov/35228754/
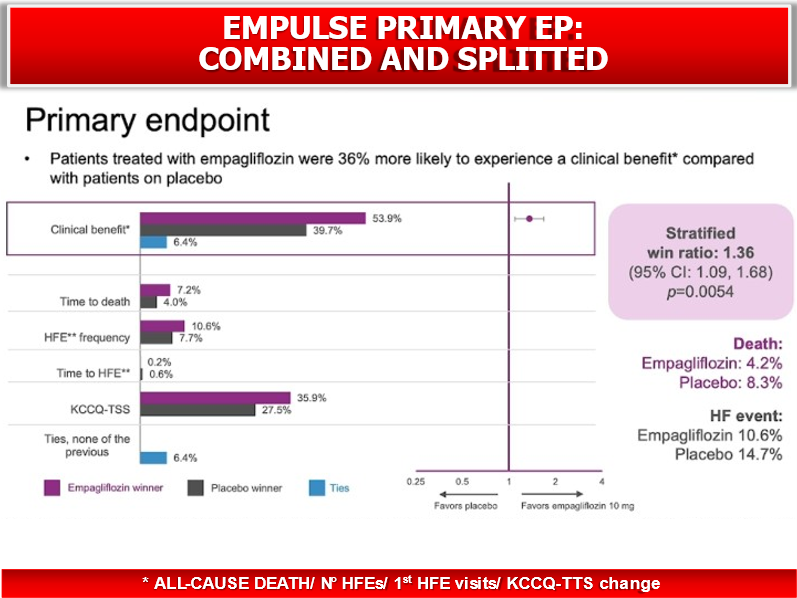
33) #EMPULSE has a particular design, using a #win_ratio to adjudicate the Primary EP. This was similar to the #ATTR_ACT trial (#tafamidis in cardiac amyloidosis). However, when considered alone the reduction of #All_cause_death + #HFE was significant.

34a) Which of the following is NOT true of a win-ratio analysis?
a. new method for examining composite endpoints
b. accounts for relative priorities of the components
c. components must be same types of outcomes
d. can incorporate quality of life #QoL scores
a. new method for examining composite endpoints
b. accounts for relative priorities of the components
c. components must be same types of outcomes
d. can incorporate quality of life #QoL scores
34b) Mark your best response and return here TOMORROW for the correct answer, a wrap-up of this #tweetorial, & a link to your 🆓CE/#CME! 👉@DjawidHashemi @DrCasanovaPablo @SeguraCardio @edurontoFF @BonanadClara @cpcannon @mvaduganathan @ShelleyZieroth @DrMarthaGulati
35) Welcome back! I am @GiuseppeGalati_ & you are earning 0.75h CE/#CME! We are discussing prevention & mgt of #HF from the #cardiologist perspective. We took a quick detour to talk about #win_ratio, a new method for examining composite endpoints, now widely adopted in #CV trials
36a) See pubmed.ncbi.nlm.nih.gov/32901285/ for a nice discussion. The answer to the quiz is C, because in fact the components of the composite #EP do NOT have to be similar. For example, the win ratio can combine the time to death with the number of occurrences of a non-fatal outcome ...
36b) ... such as CV-related hospitalizations (CVHs) in a single hierarchical composite endpoint. The win ratio can provide greater statistical power to detect and quantify a treatment difference by using all available information contained in the component outcomes.
37) So, where were we? Oh yes, trials ➡️ benefit of #SGLT2i's in #T2DM, #chronic #HFrEF, #AHF, & #CKD (the latter not covered in this edition). #SGLT2i has now been tested in #chronic #HFpEF, in #EMPEROR_PRESERVED.
Here you can see the trial design (🔓pubmed.ncbi.nlm.nih.gov/34449189/)
Here you can see the trial design (🔓pubmed.ncbi.nlm.nih.gov/34449189/)

38) #EMPEROR_PRESERVED enrolled nearly 6000 pts with the following characteristics, mean age 71.9, Female: 44.7%, NYHA II: 81%, mean LVEF:54%, #HFmREF 33%, #HFpEF (EF>50%) 33%, #HFpEF (EF>60%) 34%, median #NTproBNP: 950 pg/mL , mean #eGFR: 60 ml/min/m2


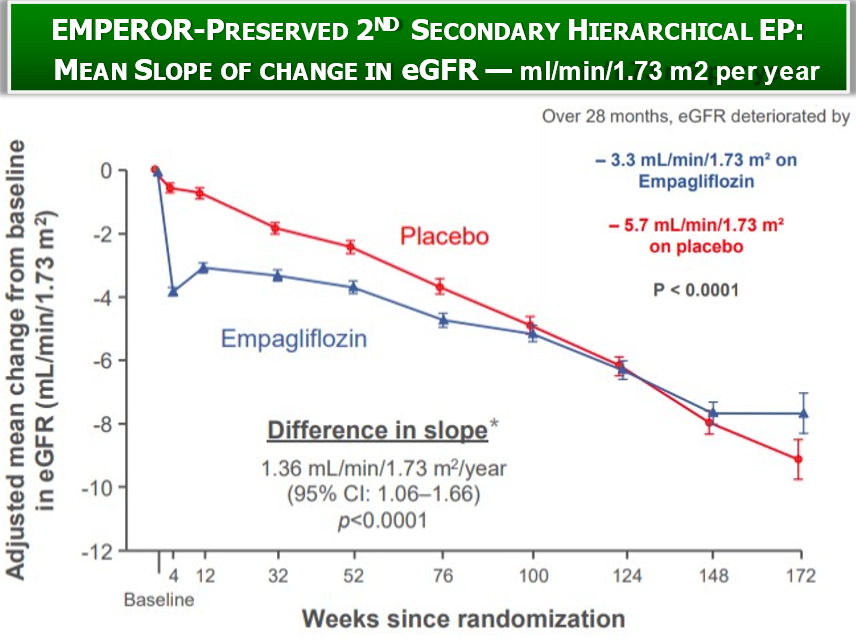
39) #EMPEROR_PRESERVED became the 1st RCT to show a significant reduction of the Primary EP: #CV_Death + 1st #HHF in #HFpEF pts (RRR:21%). Moreover, the 2nd secondary hierarchical EP was significantly reduced (Total #HHF) as well as the 2nd secondary hier. EP (eGFR mean change).


40) Beyond the significant⬇️of the 3 hierarchical EP, #empagliflozin significantly⬆️ #QoL measured by #KCCCQ. However, a harsh debate started because the reduction at a first analysis was <5 points. Therefore many not #HF physicians argued that it was not “clinically significant”

41) The 1st reply of #HFcardiologist was that #KCCCQ was built & validated in #HFrEF pts. Therefore its application to #HFpEF can’t be valued in the same manner. Further analysis of #EMPEROR_PRESERVED showed a significant⬆️of #KCCCQ especially in the domains dedicated to #QoL



42) The prespecified subgroup analysis in Primary EP did not show any difference between Diabetic vs non-diabetic patients. The ⬇️of primary #EP was significant both in #HFmrEF and in #HFpEF >50% but not in #HFpEF>60%. The last is a population that needs further study.

43) The most important criticism of #EMPEROR_PRESERVED was that in splitting the component of 1st #EP most of the benefit was driven by ⬇️of the 1st #HHF whereas⬇️#CV_Death was not significant. This analysis➡️ IIA rec to #SGLT2i in the last #ACC_AHA_HFSA guidelines

44a) But what is our real 🎯 in #HFpEF? The mean age at diagnosis of #HFpEF pts is 76 yrs, & in general all the registries of the last 20 years show advanced age at diagnosis. The mean expectancy of life in Italy (before #Covid19) was 83.5 years . . .
44b) ... (so that Italy was the 1st country in Europe & the 2nd in the globe in this stat). Therefore, from diagnosis to death in the luckiest scenario #HFpEF pts live 7 years after diagnosis.


45) So perhaps our target in #HFpEF is not to delay #CV_Death or #all_cause_death but to improve #QoL in terms of reducing #HHF, improving symptoms & functional capacity. In other words, citing Rita Levi Montalcini (Nobel Prize): Better adding life to days than days to life”

46) #CHIEF_HF (#canagliflozin in both #HFrEF & #HFpEF) and #PRESERVED_HF (#dapagliflozin in HFpEF) confirmed (removing all the residual doubts) that #SGLT2i significantly improve #QoL, #KCCCQ, #6mwt in #HFpEF pts


47) The magnitude of the benefit in term of reduction of primary #EP is even larger in real #HFpEF pts (i.e. HFpEF with LVEF>50%). Finally, we have a new #EBM drug for #HFpEF with a clear class I indication.

48) Concluding this #tweetorial, #SGLT2i have now (based on the evidence) 6⃣ indications: #TD2M, #CKD, chronic #HFrEF, chronic #HFmrEF, chronic #HFpEF, & #AHF. This justifies the title of “The statins of 21st century”! #FLOZINATE!

49) This impressive number of indications is justified by multiple mechanisms of benefit that are summarized in this review by @cardiomet_CE author @SABOURETCardio et al: “The interplay between cardiology and diabetology”
pubmed.ncbi.nlm.nih.gov/32402065/
pubmed.ncbi.nlm.nih.gov/32402065/


50) If you want to know more about #SGLT2i and #HF, please check this review in which you can find in detail the contents of this tweetorial. “Women and diabetes preventing heart disease in a new era of therapies”, 🔓 pubmed.ncbi.nlm.nih.gov/34777580/, by yours truly

51) And that's it! You made it! 0.75h CE/#CME credit 🇺🇸🇨🇦🇬🇧🇪🇺 and you can claim your certificate at cardiometabolic-ce.com/cardiorenal19/. I am @GiuseppeGalati_. Please join me in following @cardiomet_CE for the best education in #cardiometabolic medicine by expert authors, here on Twitter!
• • •
Missing some Tweet in this thread? You can try to
force a refresh












