
🧵Ever wonder what therapists use for #Suicide prevention? We asked: therapists use current best practices (~90%) BUT ~40% of clinicians endorse contracts for safety, no-harm contracts, &/or no-suicide contracts (not good!) #MentalHealthAwareness link👇 1/7 #psychtwitter 
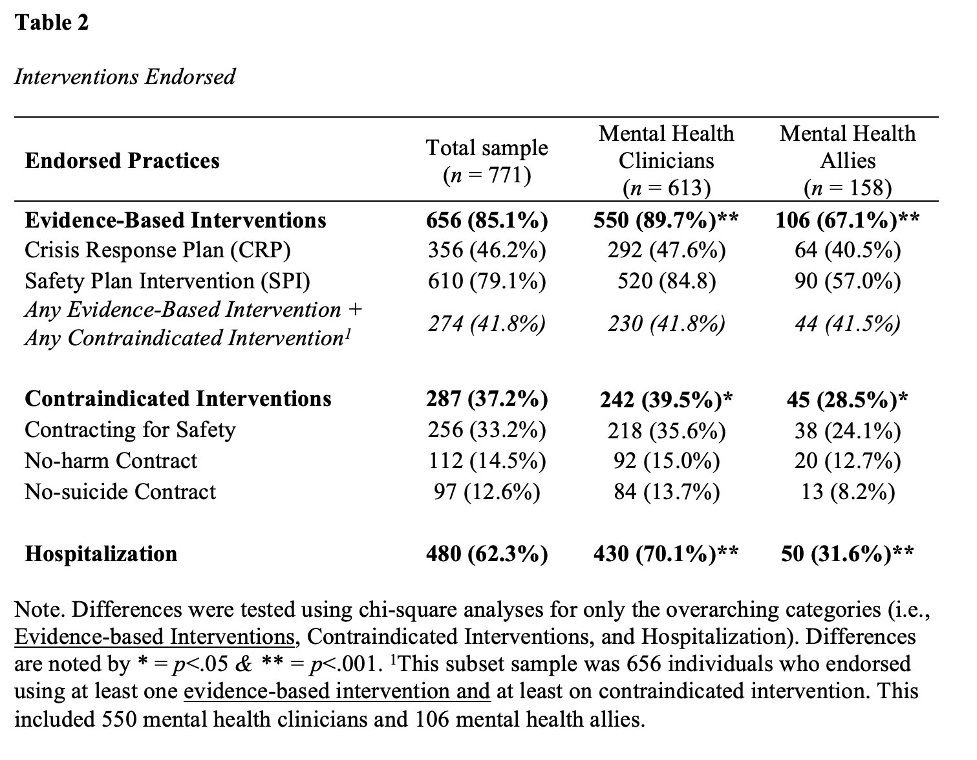
We asked mental health (MH) clinicians & MH allies (teachers, #FirstResponders, peer support) what Best Practices (Crisis Response Planning & Safety Plan) & Contraindicated Practices (contract 4 safety, no-harm contract, &/or no-suicide contract) they use. 2/7
Mental health allies endorsed the Best Practices & Contraindicated Practices at lower rates than mental health clinicians. This leaves room for more training on best practices with a focus on removing interventions that don’t help. #PeerToPeer #PeerSupport 3/7
People for this survey were asked to indicate all suicide prevention practices they use. Hospitalization was endorsed by ~70% of clinicians and only 30% of mental health allies. This is an area that could use more focus! #MentalHealthMatters #SuicidePrevention 4/7
Our takeaways are that it’s great to see high endorsement of best practices. It is worriesome to see fairly high rates of contraindicated practices. We really need to focus on #innovation and #implementation of training. There also is likely a need for de-implementation. 5/7
Some great stuff but we are far from removing old habits that don’t work. Hopefully some people believe this data (e.g., reviewers saying it is not common) and we can move forward! Link to full study 6/7: tandfonline.com/doi/abs/10.108… #MedTwitter #PsychTwitter @AcademicChatter
This was a great group of collaborators including @KatyDondanville @HannahTylerPhD @shelb_baker @Dr_John_Moring @DrJbake @ABBryan1 @craigjbryan (Twitterless Noelle Smith & Brooke Fina) @STRONGSTARTrain #StopSuicide 7/7
To make this easier @threadreaderapp #unroll
Thoughts?/might be of interest @mitchprinstein @JanelCubbage @tylerblack32 @DocRobPhD23 @__The_Nick__ @allentien @suicideresearch @socworkpodcast @JudgeWren @sspencerthomas @lab_jobes @JillHF_AFSP @UofMPastPres @afspnational @1of2vics @jack_turban @ChaseTMAnderson @SPRCtweets
• • •
Missing some Tweet in this thread? You can try to
force a refresh


