,
47 tweets,
14 min read
Read on Twitter
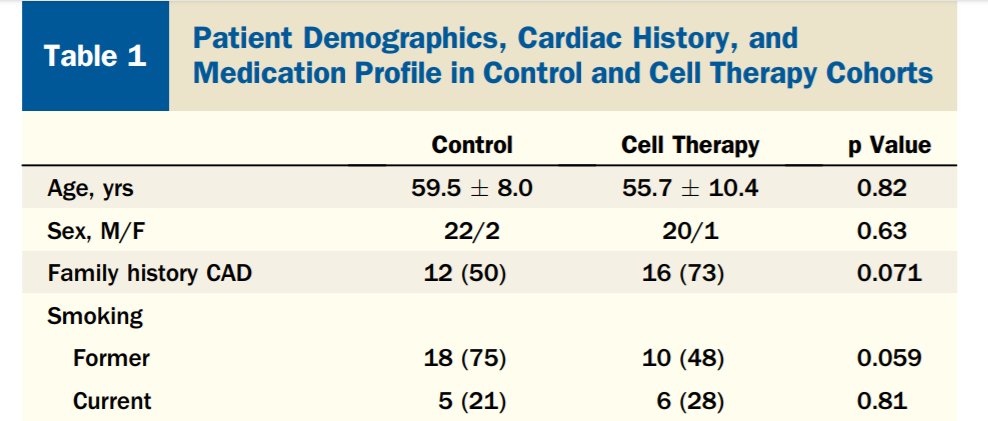
Considering #statin in 35-y-o man worried about extensive family history of MI+stroke: 2 parents, 3 of 4 sibs.
#Cholesterol 5.8 mM, 224 mg/dl. Subtypes typical for such a total.
Non-smoker. Otherwise average.
[Live-quiz from #orbita-HQ for #cardioTwitter fellows & the curious]
#Cholesterol 5.8 mM, 224 mg/dl. Subtypes typical for such a total.
Non-smoker. Otherwise average.
[Live-quiz from #orbita-HQ for #cardioTwitter fellows & the curious]
Question C2.
First vote was for diet first, and quite right too! That is the guideline, and we must obey.
Natural, organic, eco-friendly and therefore best.
What effect size is a reasonable expectation, for patient and Dr, for the reduction of total cholesterol by diet?
First vote was for diet first, and quite right too! That is the guideline, and we must obey.
Natural, organic, eco-friendly and therefore best.
What effect size is a reasonable expectation, for patient and Dr, for the reduction of total cholesterol by diet?
Question C3.
(currently 0.8 mmol/L in the lead for Question C2)
There are several ways to choose a value. Which did you use?
(currently 0.8 mmol/L in the lead for Question C2)
There are several ways to choose a value. Which did you use?
Gut instinct, in the lead at the moment, and that is good. I love it too. I always guess first, before I read the literature. That way, when I am wrong, it makes me laugh/cry: emotions that strengthen learning.
I can also tease #ORBITA hq PhD students, who'll fall into same trap
I can also tease #ORBITA hq PhD students, who'll fall into same trap
question C4.
Who was Archibald Cochrane?
A scientist who developed the warp drive?
A doctor who advocated randomized controlled trials?
A biologist who discovered statins?
A haematologist who developed a method of separating cholesterol into LDL, HDL and other bits
Who was Archibald Cochrane?
A scientist who developed the warp drive?
A doctor who advocated randomized controlled trials?
A biologist who discovered statins?
A haematologist who developed a method of separating cholesterol into LDL, HDL and other bits
Yes, the trekkies have been shrewd enough to separate Archibald from his twin brother Zefram.
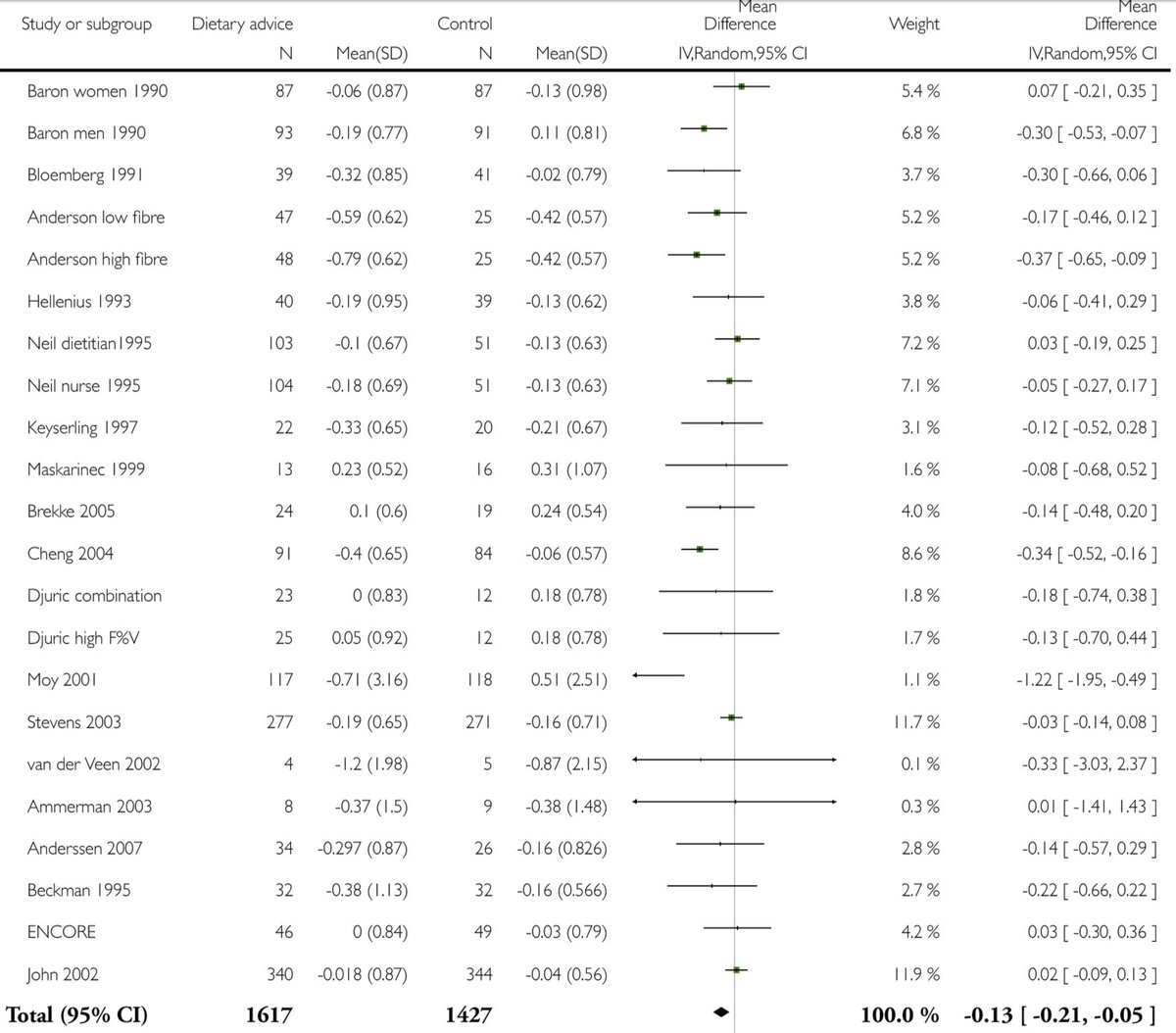
The "Cochrane Collaboration" is indeed a foundation providing syntheses of the best available evidence.
Here is there analysis on effect of diet on cholesterol.
onlinelibrary.wiley.com/doi/10.1002/14…
The "Cochrane Collaboration" is indeed a foundation providing syntheses of the best available evidence.
Here is there analysis on effect of diet on cholesterol.
onlinelibrary.wiley.com/doi/10.1002/14…
You can read the whole report for free. It is very good, but lengthy because it is meticulous.
If in a hurry, skip to page 88, or search the PDF for "Analysis 1.5".
If you are actually riding a bike or balancing on a spike in a park, so have even less time, look at this pic.
If in a hurry, skip to page 88, or search the PDF for "Analysis 1.5".
If you are actually riding a bike or balancing on a spike in a park, so have even less time, look at this pic.
Question C5.
The figure above is in mmol/l. Multiply by 40 to get mg/dl.
Based on the world total of careful RCTs, peer reviewed and reported by a variety of scientists that are not in collusion and *not* biased against diet, what is the typical effect size of diet on Chol?
The figure above is in mmol/l. Multiply by 40 to get mg/dl.
Based on the world total of careful RCTs, peer reviewed and reported by a variety of scientists that are not in collusion and *not* biased against diet, what is the typical effect size of diet on Chol?
Well I found it quite shocking.
Because I knew the answer to the following question (because I am so sad and lonely), and I realised the implications of the two facts.
Q C6
1000 men with 5.8 cholesterol (224) today have a recheck in a month. 950 of them will cover what range?
Because I knew the answer to the following question (because I am so sad and lonely), and I realised the implications of the two facts.
Q C6
1000 men with 5.8 cholesterol (224) today have a recheck in a month. 950 of them will cover what range?
First vote 5.6-6.0. Thank you! Yes we will use the fanciest machines. And pts will starve overnight, meditate, and sprinkle offerings at the feet of the statue the great god Stochaste.
You might think that this would keep them bunched up.
But! clinchem.aaccjnls.org/content/clinch…
See pic
You might think that this would keep them bunched up.
But! clinchem.aaccjnls.org/content/clinch…
See pic
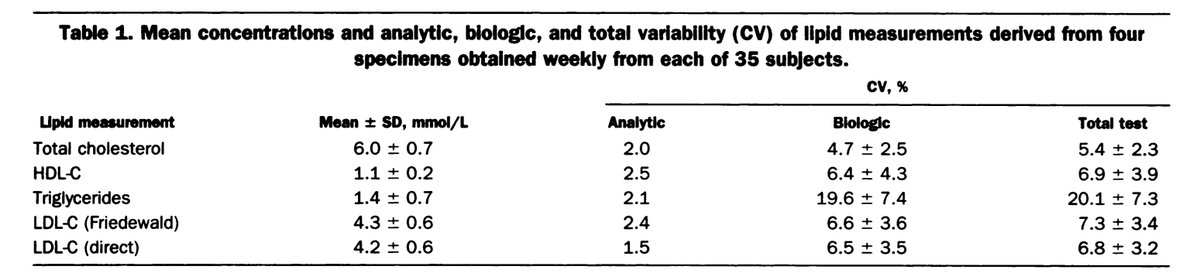
Let me focus your attention on the top row, total cholesterol.
And the right-hand column, the variability, expressed as "coefficient of variation", which means SD divided by the mean value, written as a %.
Question C7.
From this, roughly what is the SD of repeated measurements?
And the right-hand column, the variability, expressed as "coefficient of variation", which means SD divided by the mean value, written as a %.
Question C7.
From this, roughly what is the SD of repeated measurements?
ONLY READ THIS IF YOU ARE STUCK on C7.
Try and do without reading this.
Mean is 6 mM.
SD/Mean is about 5%.
SD must therefore be what?
Still stuck?
Got 20 friends.
You give each friend $30 of drinkies at your party. i.e. Total cost/nFriends=30.
How much party cost you?
Try and do without reading this.
Mean is 6 mM.
SD/Mean is about 5%.
SD must therefore be what?
Still stuck?
Got 20 friends.
You give each friend $30 of drinkies at your party. i.e. Total cost/nFriends=30.
How much party cost you?
Question C8.
Based on your calculated SD, what range do you expect 95% of values to lie in?
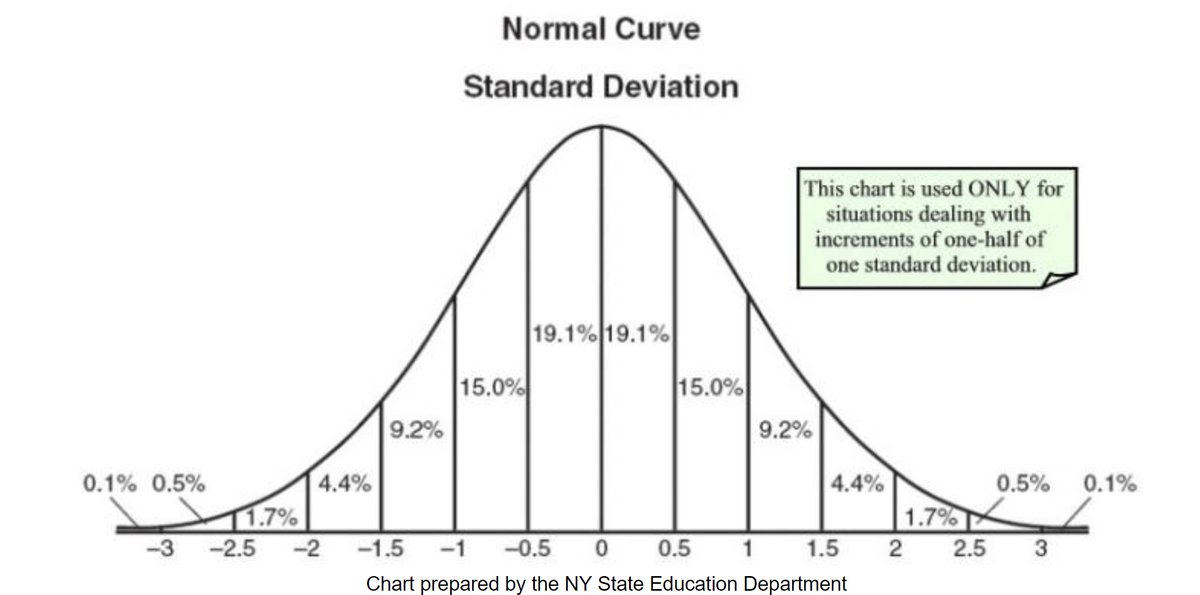
Remember, if a distribution is Normal [a future annoy-o-rama will examine what this means] about 95% of values lie within 1.96 SD of the mean. i.e. about mean-2SD to mean+2SD.
Based on your calculated SD, what range do you expect 95% of values to lie in?
Remember, if a distribution is Normal [a future annoy-o-rama will examine what this means] about 95% of values lie within 1.96 SD of the mean. i.e. about mean-2SD to mean+2SD.
Question C9, mysteriously like C6 #selfPlagiarism #soSueMe
1000 men with 5.8 cholesterol (224) today, recheck in a month. 950 will cover what range?
Don't worry if you've changed your mind. (Even if you are an interventionist and never do so)
Thinking = changing ones mind.
1000 men with 5.8 cholesterol (224) today, recheck in a month. 950 will cover what range?
Don't worry if you've changed your mind. (Even if you are an interventionist and never do so)
Thinking = changing ones mind.
Clearly not obvious...
So far, at ~10 votes, majority is right on Q7,8 and 9. So assume they are right. (#ORBITA-hq fellows - please SMS me if majority becomes wrong: "Brexit phenomenon")
Q10. Combine this with Cochrane value
Average effect of diet is what % of the "noise" SD?
So far, at ~10 votes, majority is right on Q7,8 and 9. So assume they are right. (#ORBITA-hq fellows - please SMS me if majority becomes wrong: "Brexit phenomenon")
Q10. Combine this with Cochrane value
Average effect of diet is what % of the "noise" SD?
Correct answers so far, in case getting a bit anxious.
DO NOT READ UNTIL YOU'VE TRIED.
Q7. option A.
Q8. option D.
Q9. option D.
Q10. option A.
If you can't see why, email me at d.francis@imperial.ac.uk and I will add an explanation later.
You'll need these answers for later.
DO NOT READ UNTIL YOU'VE TRIED.
Q7. option A.
Q8. option D.
Q9. option D.
Q10. option A.
If you can't see why, email me at d.francis@imperial.ac.uk and I will add an explanation later.
You'll need these answers for later.
Someone won't be taking up the offer of the Nobel prize for quantum theory, either ...
Anyway, back to what we laughingly call reality.
Q C11. Our pt gets typical benefit seen in those carefully conducted, rigorously supervised trials (indeed @rallamee calls him daily and cooks his food out of kindness because he has a sad face)
What probability next chol HIGHER?
Q C11. Our pt gets typical benefit seen in those carefully conducted, rigorously supervised trials (indeed @rallamee calls him daily and cooks his food out of kindness because he has a sad face)
What probability next chol HIGHER?
C11, above, is not easy to guess right.
Dropping ON AVERAGE by 0.15 mM, but + a noise SD of 0.30 mM. If the noise is positive and >0.15 mM (half an SD) we will be screwed: the cholesterol will rise.
Add up the areas of the bars to the right of +0.5, in mathbits.com/MathBits/TISec…
Dropping ON AVERAGE by 0.15 mM, but + a noise SD of 0.30 mM. If the noise is positive and >0.15 mM (half an SD) we will be screwed: the cholesterol will rise.
Add up the areas of the bars to the right of +0.5, in mathbits.com/MathBits/TISec…
And for the skeptical who want an independent calculation of this, try onlinestatbook.com/2/calculators/…
Mean chol drop = -0.15
SD = 0.30
Click "above" and enter "0"
Question C12.
What is the probability that after a typically well-delivered diet, cholesterol will be *higher* than pre?
Mean chol drop = -0.15
SD = 0.30
Click "above" and enter "0"
Question C12.
What is the probability that after a typically well-delivered diet, cholesterol will be *higher* than pre?
So honest, hardworking, fairminded, genuine, law-abiding doctors like Ethan Weiss @EthanJWeiss find themselves in the puzzling position of upsetting patients whom they treat according to guidelines
Q C13
How can we prevent upsetting 30% of our pts who achieve RCT-level diet and yet, through *unavoidable* natural variability, find their next chol gone the wrong way?
Do patients understand biological variability well?
Do they know relative effect sizes of diet and statin?
How can we prevent upsetting 30% of our pts who achieve RCT-level diet and yet, through *unavoidable* natural variability, find their next chol gone the wrong way?
Do patients understand biological variability well?
Do they know relative effect sizes of diet and statin?
Q C14.
If they find all of this difficult to cope with, what else can we do to help them achieve lower cholesterols?
If they find all of this difficult to cope with, what else can we do to help them achieve lower cholesterols?
I do all 3 with my patients.
It may be in contravention of guidelines, but I am ready to explain my reasoning along the above lines.
I am not against diet, I just don't want to set the patient up for a fall.
So statin from day 1, with diet, recheck only on both.
It may be in contravention of guidelines, but I am ready to explain my reasoning along the above lines.
I am not against diet, I just don't want to set the patient up for a fall.
So statin from day 1, with diet, recheck only on both.
I have to congratulate @DLBhattMD, the great peacemaker!
A sentence so ingeniously worded that, against all my baser instincts, I am forced to agree with @GreggWStone agreeing with you, as there is no logical way out of an NSTEMI being a STEMI without STE.
A sentence so ingeniously worded that, against all my baser instincts, I am forced to agree with @GreggWStone agreeing with you, as there is no logical way out of an NSTEMI being a STEMI without STE.
Question C15.
Let's put the 0.15mM (6 mg/dl) effects of diet into context. What effect size would you expect on average from (say) atorva 40mg, with starting cholesterol 5.8 mM (224 mg/dl)?
Let's put the 0.15mM (6 mg/dl) effects of diet into context. What effect size would you expect on average from (say) atorva 40mg, with starting cholesterol 5.8 mM (224 mg/dl)?
Information that may help on C15.
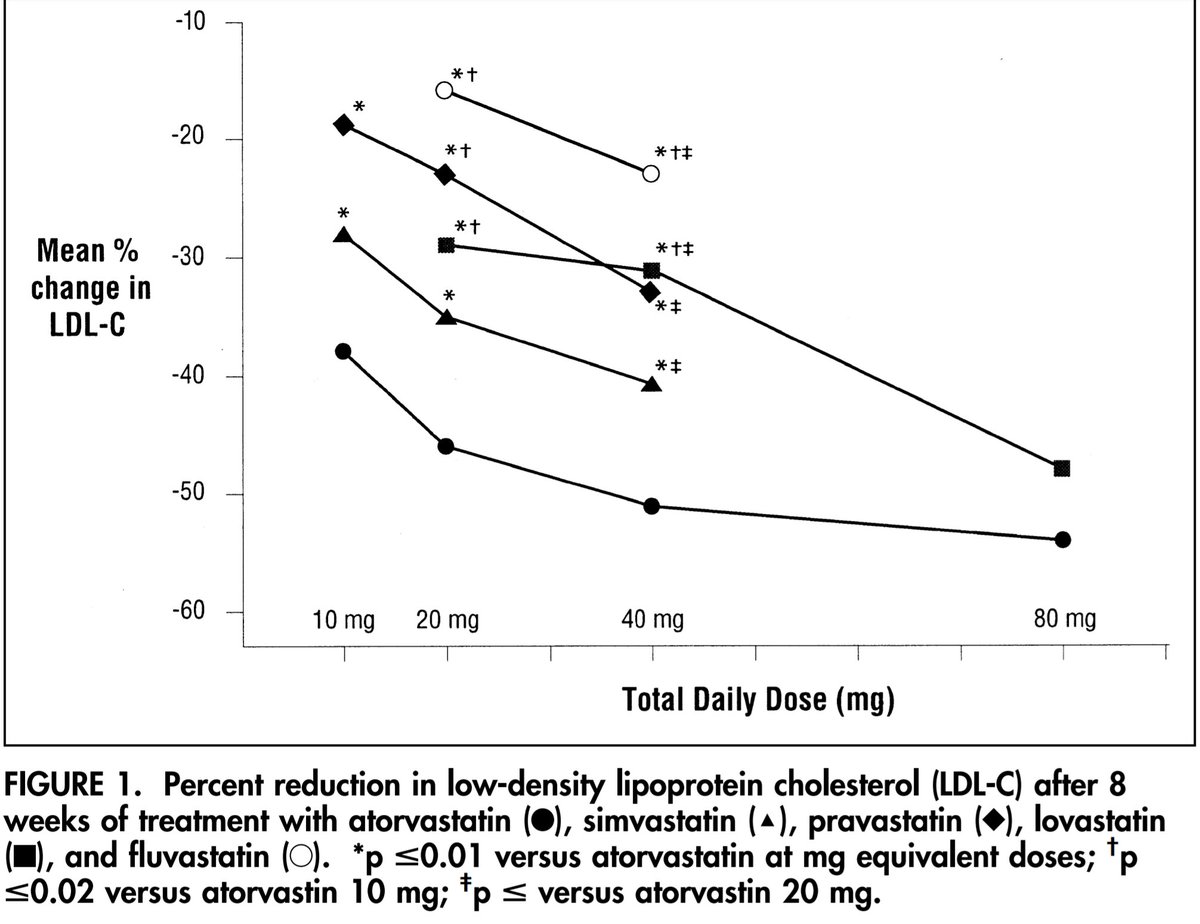
Here is a CURVES study graph (admittedly plotting LDL-cholesterol, not total cholesterol) showing effect sizes as a percentage of baseline.
Suppose the non-LDL cholesterol was about 2mM, so:
LDL was 3.8 mM (147 mg/dl)
ncbi.nlm.nih.gov/pubmed/9514454
Here is a CURVES study graph (admittedly plotting LDL-cholesterol, not total cholesterol) showing effect sizes as a percentage of baseline.
Suppose the non-LDL cholesterol was about 2mM, so:
LDL was 3.8 mM (147 mg/dl)
ncbi.nlm.nih.gov/pubmed/9514454
Perhaps some confusion on C15
Q C16.
Look at the graph above.
40mg of atorvastatin (solid round blobs) reduces LDL-C by what %?
Q C16.
Look at the graph above.
40mg of atorvastatin (solid round blobs) reduces LDL-C by what %?
Now that's better!
Q C17.
We estimated our guy's LDL-C to be 3.8mM
So, based on the percentage you read off the graph, what will be the absolute (i.e. in mM, not %) fall in LDL-C?
Q C17.
We estimated our guy's LDL-C to be 3.8mM
So, based on the percentage you read off the graph, what will be the absolute (i.e. in mM, not %) fall in LDL-C?
Aside from LDL, there is other stuff in the total cholesterol, for example HDL.
Dan Keene ruined any interest I had in raising HDL: bmj.com/content/bmj/34…
"One agent for increasing HDL, torcetrapib, did significantly
change mortality, but [unfortunately] this was an increase."
Dan Keene ruined any interest I had in raising HDL: bmj.com/content/bmj/34…
"One agent for increasing HDL, torcetrapib, did significantly
change mortality, but [unfortunately] this was an increase."
Q C18.
So taking Dan's cue, let's cross our fingers and assume that HDL (and other things other than LDL) are unaffected.
Roughly what change will we expect in total cholesterol, therefore?
So taking Dan's cue, let's cross our fingers and assume that HDL (and other things other than LDL) are unaffected.
Roughly what change will we expect in total cholesterol, therefore?
Q C19.
And so what is the approximate ratio between:
the effect size of 40mg of generic atorvastatin (UK price approx 5 US cents/day)
and
the effect size of a high-quality, RCT level supervision (@rallamee on speed dial) diet?
And so what is the approximate ratio between:
the effect size of 40mg of generic atorvastatin (UK price approx 5 US cents/day)
and
the effect size of a high-quality, RCT level supervision (@rallamee on speed dial) diet?
Let's think about whom we recommend statins to.
Perhaps you quantify CV risk and recommend statins to those at highest risk?
Or maybe you don't formally calculate risk in % over 10 years or whatever, but just mentally gauge it?
Q C20.
Initiating statins is most beneficial in:
Perhaps you quantify CV risk and recommend statins to those at highest risk?
Or maybe you don't formally calculate risk in % over 10 years or whatever, but just mentally gauge it?
Q C20.
Initiating statins is most beneficial in:
"Highest risk" is ahead in the polls.
Of course, it's so obvious we never question it.
But there is always a nasty sting in any of my questions that seem too easy, as you will by now have noticed. 🤓
Here the trap is that I didn't say what I meant by "most beneficial".
Of course, it's so obvious we never question it.
But there is always a nasty sting in any of my questions that seem too easy, as you will by now have noticed. 🤓
Here the trap is that I didn't say what I meant by "most beneficial".
I worry that the first 6 votes on C19 are producing this.
I am asking you to divide 1.9 mM by 0.15 mM.
I was hoping you could guess, e.g. is it going to be more or less than 10. But if you find that tricky, just use a calculator.
I am asking you to divide 1.9 mM by 0.15 mM.
I was hoping you could guess, e.g. is it going to be more or less than 10. But if you find that tricky, just use a calculator.
OK back to whom we are giving statins to.
C21.
By "beneficial", which of these could I have meant?
C21.
By "beneficial", which of these could I have meant?
Question C22.
Which of these quantities is most familiar to patients?
Think about whether the quantity is commonly talked about in general conversation.
Think what the unit of measurement is. Something tangible?
Depends on an arbitrary time window? Or covers all of time?
Which of these quantities is most familiar to patients?
Think about whether the quantity is commonly talked about in general conversation.
Think what the unit of measurement is. Something tangible?
Depends on an arbitrary time window? Or covers all of time?
"Years of life" is in the lead.
Everyone has heard of them; everyone wants them.
My friend Marianna Fontana, Cardiac MR guru at Royal Free, calculated life years gained from statins. circ.ahajournals.org/content/129/24…
Look at the plot carefully
ncbi.nlm.nih.gov/pmc/articles/P…
(Low res pic here)
Everyone has heard of them; everyone wants them.
My friend Marianna Fontana, Cardiac MR guru at Royal Free, calculated life years gained from statins. circ.ahajournals.org/content/129/24…
Look at the plot carefully
ncbi.nlm.nih.gov/pmc/articles/P…
(Low res pic here)
Above was Marianna's "Paddington plot" of LIFE MONTHS GAINED from starting a statin, for either sex, at any BP and cholesterol level.
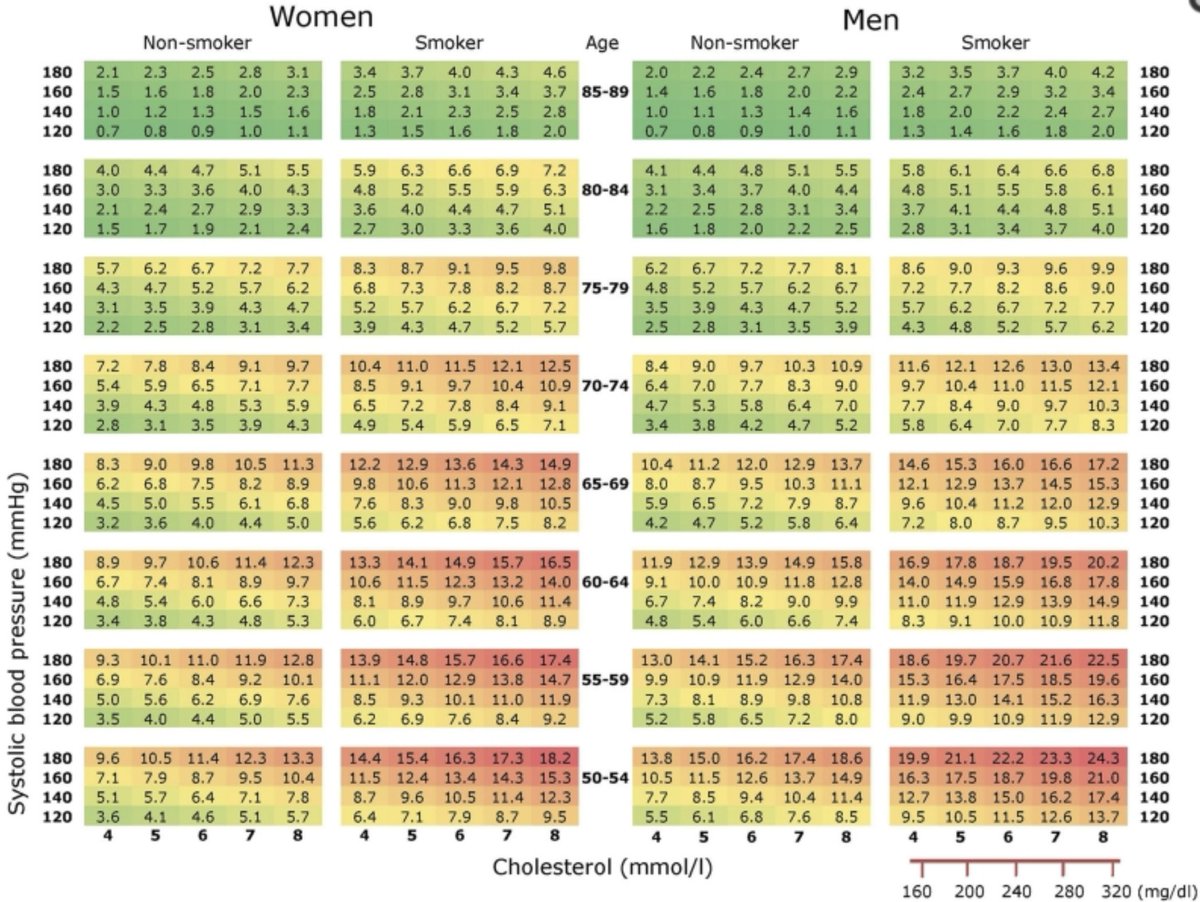
Below is the more familiar SCORE chart of risk. It is part of our European guideline and on every UK Dr's desk in the "BNF" drugs book.
Compare.
Below is the more familiar SCORE chart of risk. It is part of our European guideline and on every UK Dr's desk in the "BNF" drugs book.
Compare.
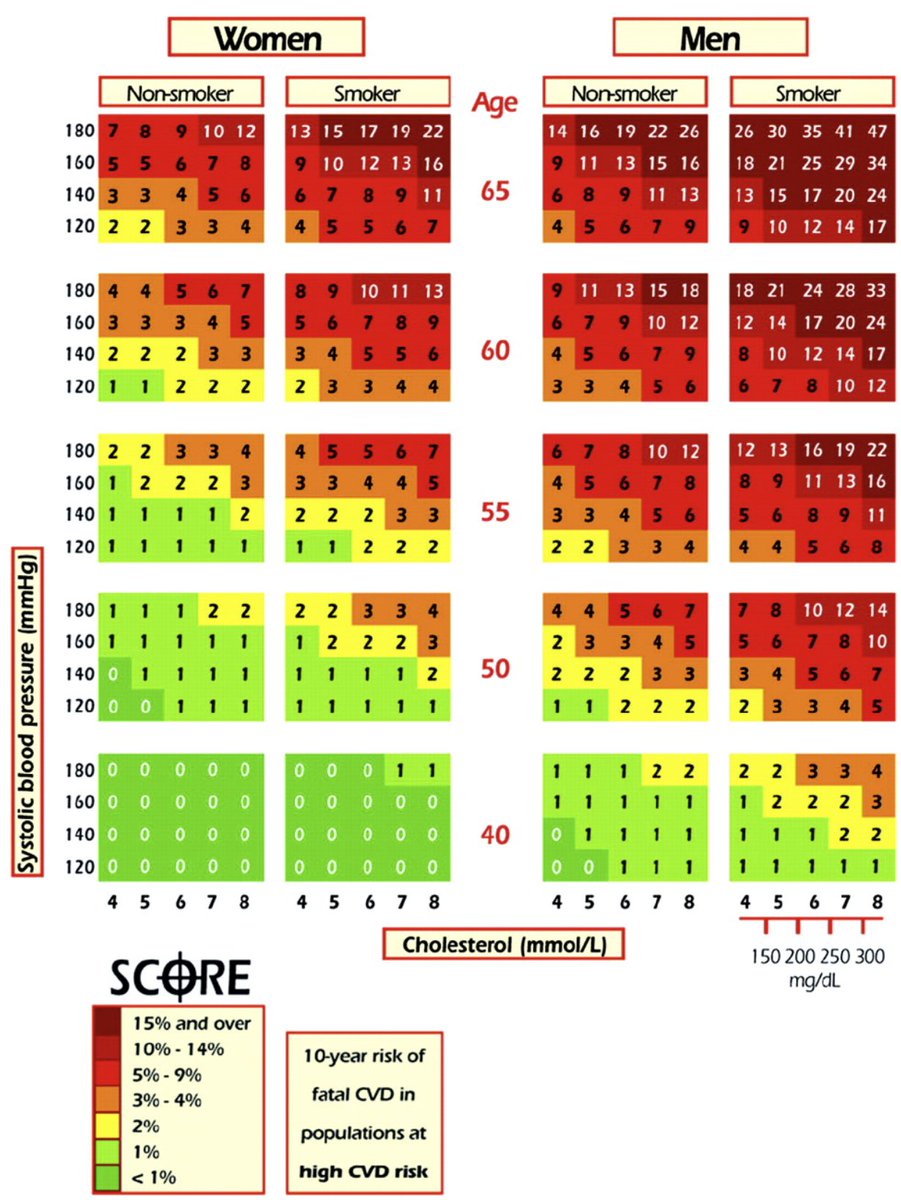
The SCORE chart correctly shows that *10-y-risk* goes up with male sex, cholesterol, blood pressure, and age.
Marianna's chart, of *life years gained from starting a statin* differs in only one way, other than having a less screamy colour scheme.
How does Marianna's LYG differ?
Marianna's chart, of *life years gained from starting a statin* differs in only one way, other than having a less screamy colour scheme.
How does Marianna's LYG differ?
Q C24.
Both first responders are correct, thank you!
Of course Marianna's plot doesn't fail to do anything. It just reflects something that is obvious (in retrospect).
But not a big feature of guidelines.
Both first responders are correct, thank you!
Of course Marianna's plot doesn't fail to do anything. It just reflects something that is obvious (in retrospect).
But not a big feature of guidelines.
Q C25.
Your STEMI patients go straight onto statins, yes?
Now think of your last 20 *primary prevention* statin initiations, instead. Remember the discussions about diet, lifestyle and meds?
Remember the to-and-fro?
Denial/anger/bargaining/acceptance?
What upset patients most?
Your STEMI patients go straight onto statins, yes?
Now think of your last 20 *primary prevention* statin initiations, instead. Remember the discussions about diet, lifestyle and meds?
Remember the to-and-fro?
Denial/anger/bargaining/acceptance?
What upset patients most?
First response is "Deciding yes or no". That is what I have seen too. The initial decision can take months or years, with extensive use of lay referral network, to-and-fro of newspaper cuttings, reports that grandma made ill by statins, etc.
Once initiated, things go much more smoothly. The key is to have a correctly informed patient (more on this later in this thread!)
So I argue that the major displeasure to patients of being on the statin is getting over that initial hurdle of trying the damn things.
So I argue that the major displeasure to patients of being on the statin is getting over that initial hurdle of trying the damn things.
If my assertion is true, that the upfront irritation is the main "disutility" of a statin, then this is roughly the same at any age. [Marianna's paper surveys hundreds of people and finds this too].
Therefore the net benefit (utility minus disutility) is greatest at younger ages
Therefore the net benefit (utility minus disutility) is greatest at younger ages
Therefore I assert that the patients who benefit the most (in terms of life years gained) are *not* those at highest risk, who are the very oldest (top of SCORE charts, bright shouty red)
but those at the bottom of the age spectrum.
Their large LYG comes from their youth.
Q C26
but those at the bottom of the age spectrum.
Their large LYG comes from their youth.
Q C26
I am going to have a ~1 hour gap to about 2130 GMT. Please anyone with any questions/comments, put them as a reply here (reply to the last person who spoke, so all can be in the thread). I would be grateful if people who put side comments earlier, delete them and add here. Ta, DF