
@jamesfomahony @mikey0callaghan @ESRIDublin 1./
Hi Guys, Post another crazy afternoon in GP land.
I'll make points as I read this paper:
From the start it's looking like a much more thoughtful analysis than the 2016 ESRI discussion document and 2015 HSE vs Yvonne Williams documents.
Hi Guys, Post another crazy afternoon in GP land.
I'll make points as I read this paper:
From the start it's looking like a much more thoughtful analysis than the 2016 ESRI discussion document and 2015 HSE vs Yvonne Williams documents.
@jamesfomahony @mikey0callaghan @ESRIDublin 2./
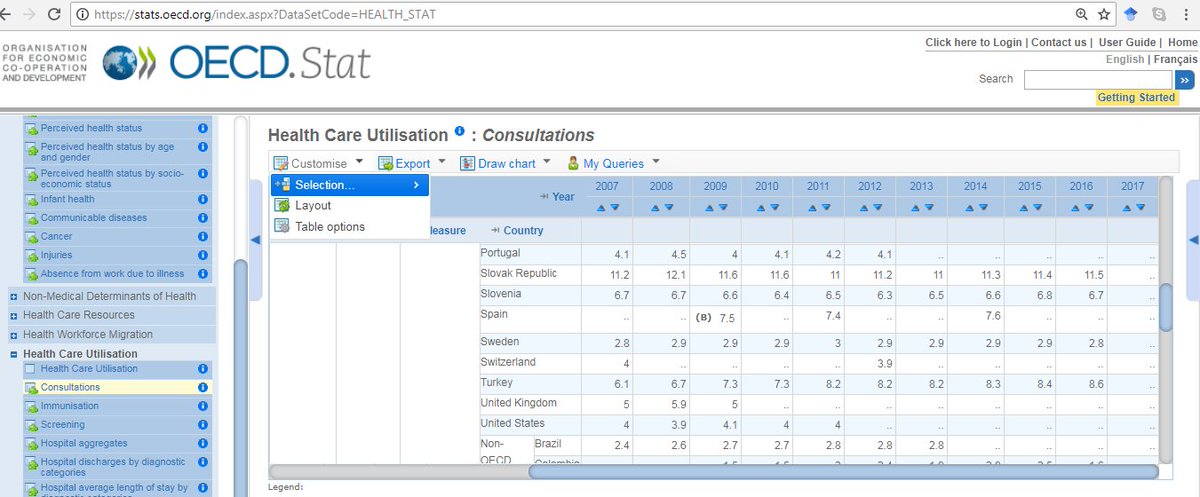
GP fees €50 per visit: From a purchaser perspective the headline rate attracts attention but from @OECD_Stat and supplier perspective the average is more reliable
GP fees €50 per visit: From a purchaser perspective the headline rate attracts attention but from @OECD_Stat and supplier perspective the average is more reliable
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat 3./
Good theoretical point on barriers to GPVC based on income deter less frequent GP attenders: potentially inflating current GPVC attendance rate however not sure if @AnnFamMed @mikey0callaghan data supports that for U6 popltn
(I believe that U6 activity influences Rnot=adult)
Good theoretical point on barriers to GPVC based on income deter less frequent GP attenders: potentially inflating current GPVC attendance rate however not sure if @AnnFamMed @mikey0callaghan data supports that for U6 popltn
(I believe that U6 activity influences Rnot=adult)
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed 4./
Disparity of chronic illness between holders/non-holders of medical cards is obvious b/c MC popltn = older,poorer & sicker
BUT
Aren't the more affluent more likely to attend for chronic disease management than less affluent if everything is equal (GP free at source)?
Disparity of chronic illness between holders/non-holders of medical cards is obvious b/c MC popltn = older,poorer & sicker
BUT
Aren't the more affluent more likely to attend for chronic disease management than less affluent if everything is equal (GP free at source)?
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed 5./
Gotcha!
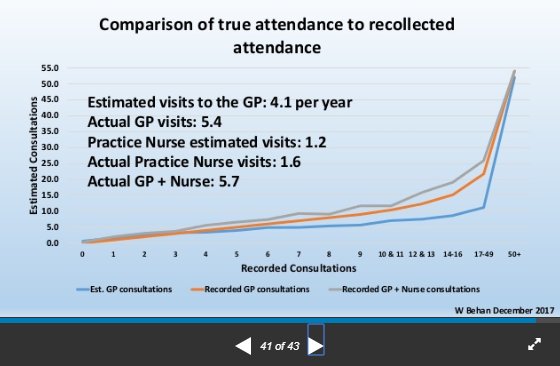
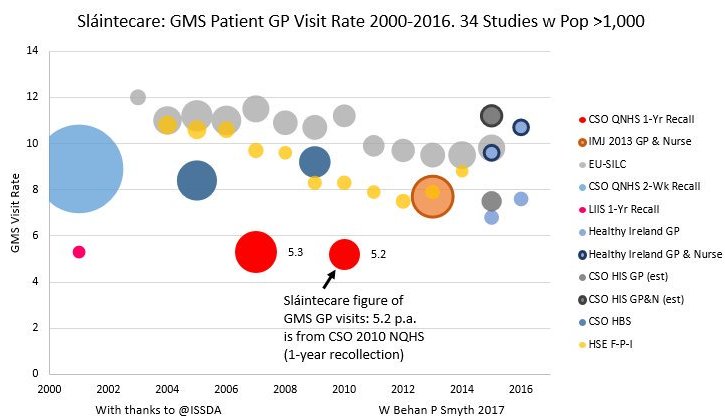
1-year survey GP visiting rate data:
The patient answer to "how many times have you attended your GP in the last 12 months" is subjected to significant degradation of recollection w time
BUT......
Gotcha!
1-year survey GP visiting rate data:
The patient answer to "how many times have you attended your GP in the last 12 months" is subjected to significant degradation of recollection w time
BUT......

@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed 6./
Answers to the binomial question "Have you attended your GP in the last 12 months" iare really reliable:
We found in our 873 patient/16 practice survey
-96% of patient responses = EMR
-2.4% forgot attending their GP in the last year
-1.4% were wrong when they said they had
Answers to the binomial question "Have you attended your GP in the last 12 months" iare really reliable:
We found in our 873 patient/16 practice survey
-96% of patient responses = EMR
-2.4% forgot attending their GP in the last year
-1.4% were wrong when they said they had
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed 7./
=> Our 2013 method of calculating true private patient visit rates is reliable
We used individual raw practice mid-year GMS popltn data to clarify what proportion GMS population truly attended
We balanced GMS patients who went elsewhere w temporary GMS who visited(?3% visits)
=> Our 2013 method of calculating true private patient visit rates is reliable
We used individual raw practice mid-year GMS popltn data to clarify what proportion GMS population truly attended
We balanced GMS patients who went elsewhere w temporary GMS who visited(?3% visits)
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed 8./
"McGovern (2015) estimates that extending free GP care to all in 2015 => an increase in the number of GP visits by 23%" is higher than 2013 Behan et al estimate of 18%
NB
Recent @ESRIDublin data suggests 2014 GP activity is 0.2% different to Behan analysis same demographics
"McGovern (2015) estimates that extending free GP care to all in 2015 => an increase in the number of GP visits by 23%" is higher than 2013 Behan et al estimate of 18%
NB
Recent @ESRIDublin data suggests 2014 GP activity is 0.2% different to Behan analysis same demographics
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed 9./
Note McGovern makes no effort to the exponential growth in GP complexity and workload as is mirrored in other jurisdictions allied to the progressive failure of secondary services to support us thus under-estimating increase in future workload
Note McGovern makes no effort to the exponential growth in GP complexity and workload as is mirrored in other jurisdictions allied to the progressive failure of secondary services to support us thus under-estimating increase in future workload
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed 10./
True, our 6 practices were not a random sample
BUT
a. We could stand over the quality of the data we produced
b. Charles Cannel stated non-selection biases have a greater effect than selection biases on reliability GP visit data
c. We were 0.2% different v @HealthyIreland
True, our 6 practices were not a random sample
BUT
a. We could stand over the quality of the data we produced
b. Charles Cannel stated non-selection biases have a greater effect than selection biases on reliability GP visit data
c. We were 0.2% different v @HealthyIreland

@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland 11./
This alone merits a long thread.
Catch up later.
Have a good weekend all!
This alone merits a long thread.
Catch up later.
Have a good weekend all!
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland 12./
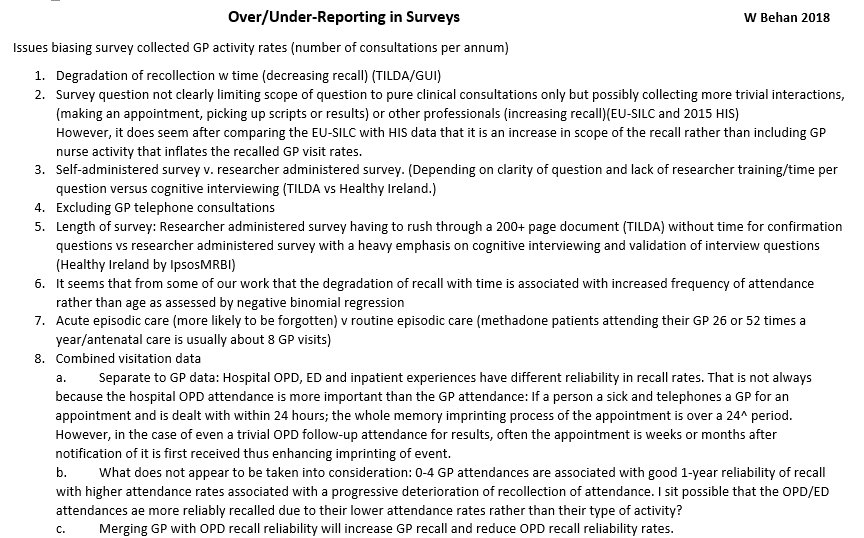
GUI Survey methodology biases include:
1. Proxy recollection which is a/w a 20% degradation according to Cannel
2. 1-year recall(a/w significant under-recollection GP visits in adults)
3. Wave 1 reports GP nurse visits as PHN visits
Gorecki knows this
irisheconomy.ie/index.php/2015…
GUI Survey methodology biases include:
1. Proxy recollection which is a/w a 20% degradation according to Cannel
2. 1-year recall(a/w significant under-recollection GP visits in adults)
3. Wave 1 reports GP nurse visits as PHN visits
Gorecki knows this
irisheconomy.ie/index.php/2015…
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed Correction: "true private patient visit rates" should read "true GMS/GPVC visit rates"
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland 13./
True: GUI, TILDA, QNHS & SILC are all random populations and Behan 2013 isn't, but Gorecki is dismissing all the biases a/w 1-year survey data (see below)
TILDA does NOT use cognitive interviewing to the level that Healthy Ireland does (Same researchers run both surveys)....
True: GUI, TILDA, QNHS & SILC are all random populations and Behan 2013 isn't, but Gorecki is dismissing all the biases a/w 1-year survey data (see below)
TILDA does NOT use cognitive interviewing to the level that Healthy Ireland does (Same researchers run both surveys)....
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland 14./
Cleary and Jette 1984 is Goreckis main defense of the reliability of patient 1-year recall of GP visiting.
He previously references it in the @HSELive v Yvonne Williams case
So lets look at how it stands up to scrutiny....
Cleary and Jette 1984 is Goreckis main defense of the reliability of patient 1-year recall of GP visiting.
He previously references it in the @HSELive v Yvonne Williams case
So lets look at how it stands up to scrutiny....
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive 15./
a. Does C&J 1984 measure general practice activity?
Reference 13.: Mechanic D, Greenley JR, Cleary PD, et al.
A model of rural health care: consumer response among users of the Marshfield Clinic
Med Care 1980; 18:597
Measures a 159 Doctor clinic....
a. Does C&J 1984 measure general practice activity?
Reference 13.: Mechanic D, Greenley JR, Cleary PD, et al.
A model of rural health care: consumer response among users of the Marshfield Clinic
Med Care 1980; 18:597
Measures a 159 Doctor clinic....
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive 16./
Of the 159 clinic doctors, we know that GPs were in 4 satellite clinics and possibly not audited: Audit was of OPD recollection which is more reliable than 1-year recall of GP attendance
So clearly the wrong 1984 US activity is being used to support Irish GP survey data....
Of the 159 clinic doctors, we know that GPs were in 4 satellite clinics and possibly not audited: Audit was of OPD recollection which is more reliable than 1-year recall of GP attendance
So clearly the wrong 1984 US activity is being used to support Irish GP survey data....
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive 17./
b. If you check the activity rates for the Marshfield clinic, they are much lower that what the prevailing national CDC figures were for that period:
cdc.gov/nchs/data/seri…
Further supporting view that C&J 1984 is missing GP data
AND
Lower visit rates = better recall....
b. If you check the activity rates for the Marshfield clinic, they are much lower that what the prevailing national CDC figures were for that period:
cdc.gov/nchs/data/seri…
Further supporting view that C&J 1984 is missing GP data
AND
Lower visit rates = better recall....
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive 18./
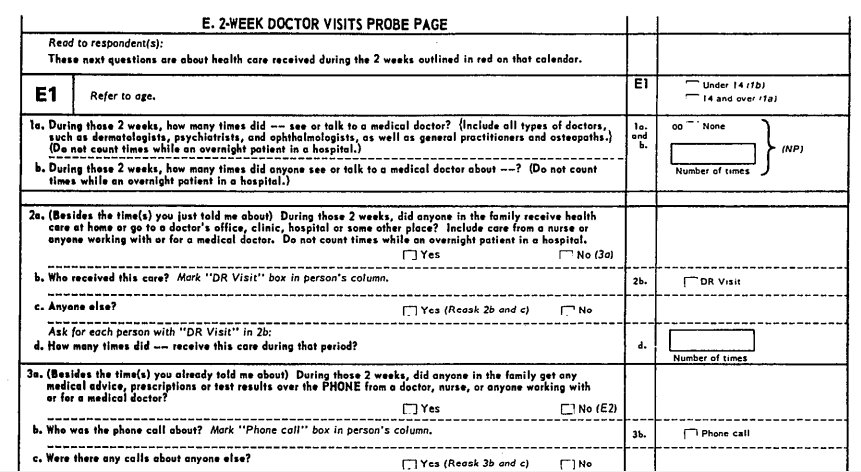
CDC used 2-week recall for its National Health Interview Survey 1962 until recently:
A summary of research studies of interviewing methodology, 1959-1970. Cannell, C.
(Vital and health statistics: Series 2, Data evaluation & methods research; no. 69)
cdc.gov/nchs/data/seri…
CDC used 2-week recall for its National Health Interview Survey 1962 until recently:
A summary of research studies of interviewing methodology, 1959-1970. Cannell, C.
(Vital and health statistics: Series 2, Data evaluation & methods research; no. 69)
cdc.gov/nchs/data/seri…
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive 19./
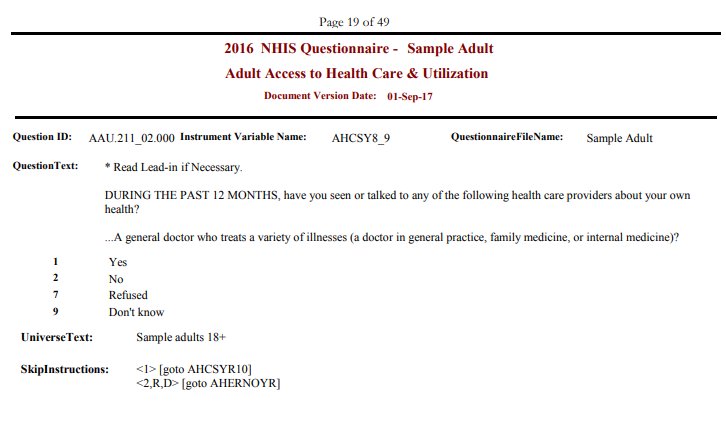
More recent US HIS questionnaires use 1-year recall data for adults and children (but 2-week for family) doctor visits
cdc.gov/nchs/nhis/data…
but that has not accepted by @EU_Eurostat since 2011 which has been supporting 4-week recall for doctor visit surveys since 2006...
More recent US HIS questionnaires use 1-year recall data for adults and children (but 2-week for family) doctor visits
cdc.gov/nchs/nhis/data…
but that has not accepted by @EU_Eurostat since 2011 which has been supporting 4-week recall for doctor visit surveys since 2006...
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat 20./
Gorecki is clearly conflating 2 two different 1-year recall concepts here:
a. Recall requiring a binary response +
b. Recall requiring a continuous (scale) response
a. Is very reliable (yes/no answer)
b. Is reliable for low but unreliable for high GP visiting rates...
Gorecki is clearly conflating 2 two different 1-year recall concepts here:
a. Recall requiring a binary response +
b. Recall requiring a continuous (scale) response
a. Is very reliable (yes/no answer)
b. Is reliable for low but unreliable for high GP visiting rates...

@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat 21./
"This paper does not directly discuss recent estimates of baseline GP care in Ireland"
Because they mirror Behan et al 2013 data to within 0.2% accuracy if 2014 demographics are applied to 2013 Behan et al data?
But...
"This paper does not directly discuss recent estimates of baseline GP care in Ireland"
Because they mirror Behan et al 2013 data to within 0.2% accuracy if 2014 demographics are applied to 2013 Behan et al data?
But...

@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat 22./
we will promote 1-year recall @tilda_tcd #GUI and 2007 + 2010 @CSOIreland #NQHS surveys which produce figures that suit government policy
So we will ignore @EU_Eurostat backed 4-week recall @CSOIreland EU-SILC 2003-2015, #HIS and @roinnslainte @HealthyIreland @IpsosMRBI data
we will promote 1-year recall @tilda_tcd #GUI and 2007 + 2010 @CSOIreland #NQHS surveys which produce figures that suit government policy
So we will ignore @EU_Eurostat backed 4-week recall @CSOIreland EU-SILC 2003-2015, #HIS and @roinnslainte @HealthyIreland @IpsosMRBI data

@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 33./
The 1-year recall Living in Ireland Survey(LIIS) was the Irish version of the European Community Household Panel (ECHP) 1995-2001
It collected GP visiting data on both public + private patients and was a precursor to 4-week recall EU-SILC 2003-2016 (collected GMS data only)
The 1-year recall Living in Ireland Survey(LIIS) was the Irish version of the European Community Household Panel (ECHP) 1995-2001
It collected GP visiting data on both public + private patients and was a precursor to 4-week recall EU-SILC 2003-2016 (collected GMS data only)
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 24./
How it is amazing that an annual 2003-2015 @CSOIreland survey w 8-15,000 participants is ignored in favor of a 2001 survey w 7,000 participants.
Is it because that data it provides is a much higher GP visiting rate than in Behan et al 2013 and therefor does not suit?
How it is amazing that an annual 2003-2015 @CSOIreland survey w 8-15,000 participants is ignored in favor of a 2001 survey w 7,000 participants.
Is it because that data it provides is a much higher GP visiting rate than in Behan et al 2013 and therefor does not suit?
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 25./
Collusion of incompetents?
Gorecki refers to Wren et al. esri.ie/publications/a… To support his thesis that Behan et al. 2013
a. Overestimates baseline GP attendance
b. Overestimates increase in GP activity associated w free universal GP care
Reliance on C&J 1984 see 14./
Collusion of incompetents?
Gorecki refers to Wren et al. esri.ie/publications/a… To support his thesis that Behan et al. 2013
a. Overestimates baseline GP attendance
b. Overestimates increase in GP activity associated w free universal GP care
Reliance on C&J 1984 see 14./
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 26./
Gorecki supports Wren et al. 2015 suggestion of an annual increase in GP visits by 18.2%
But he considers the Behan et al. 2013 suggested increase of 18.2% in GP visit rates IF WORK PRACTICES WERE TO REMAIN THE SAME as unreliable (28.6m/24.3m)
archive.imj.ie/ViewArticleDet…
Daft!
Gorecki supports Wren et al. 2015 suggestion of an annual increase in GP visits by 18.2%
But he considers the Behan et al. 2013 suggested increase of 18.2% in GP visit rates IF WORK PRACTICES WERE TO REMAIN THE SAME as unreliable (28.6m/24.3m)
archive.imj.ie/ViewArticleDet…
Daft!
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 27./
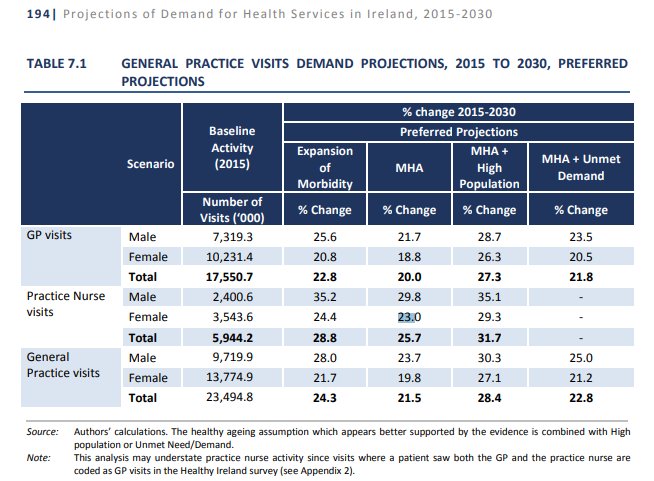
Gorecki considers Wren et al 2015 pg 33 assessment of GP workload 13.68 million consultations (GP only) as reliable and Behan et al 2013 figures unreliable
Despite Wren et al 2017 figure of 23.5 million GP + Nurse visits (2014 demographics) being 0.2% different to 2013 Behan
Gorecki considers Wren et al 2015 pg 33 assessment of GP workload 13.68 million consultations (GP only) as reliable and Behan et al 2013 figures unreliable
Despite Wren et al 2017 figure of 23.5 million GP + Nurse visits (2014 demographics) being 0.2% different to 2013 Behan

@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 28./
Gorecki consistently ignores new @ESRIDublin and @mikey0callaghan @AnnFamMed analysis that supports my assessments in favor of historical 1-year recall, no GP nurse activity data that suggests a much lower GP activity rates
GP Nurses do in 2018 a lot of what GPs did in 1972
Gorecki consistently ignores new @ESRIDublin and @mikey0callaghan @AnnFamMed analysis that supports my assessments in favor of historical 1-year recall, no GP nurse activity data that suggests a much lower GP activity rates
GP Nurses do in 2018 a lot of what GPs did in 1972
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 28./
So Behan et al. 2013 is found to produce the most reliable 2014 GP activity rates (0.2% different) and the most reliable change in overall workload (exactly the same 18.2%) compared to 2018 @ESRIDublin data esri.ie/pubs/RB201813.… but Gorecki dismisses it as unreliable
So Behan et al. 2013 is found to produce the most reliable 2014 GP activity rates (0.2% different) and the most reliable change in overall workload (exactly the same 18.2%) compared to 2018 @ESRIDublin data esri.ie/pubs/RB201813.… but Gorecki dismisses it as unreliable
@jamesfomahony @mikey0callaghan @ESRIDublin @OECD_Stat @AnnFamMed @HealthyIreland @HSELive @EU_Eurostat @tilda_tcd @CSOIreland @roinnslainte @IpsosMRBI 29./
And he compounds his under-reflection of the future GP workload by not taking into account the
a. Massive increase in complexity in GP care for routine activity
b. Increase in planned chronic disease management
c. Planned extra services and
d. Changing national demographics
And he compounds his under-reflection of the future GP workload by not taking into account the
a. Massive increase in complexity in GP care for routine activity
b. Increase in planned chronic disease management
c. Planned extra services and
d. Changing national demographics












