
I’m going to throw my hat in the Tweetorial ring.
Sometimes salt tablets work for hyponatremia and sometimes they don’t. How can you figure out when to use them and when not to?
Sometimes salt tablets work for hyponatremia and sometimes they don’t. How can you figure out when to use them and when not to?
The kidney regulates total body sodium and total body water independently. The renin angiotensin aldosterone system regulates total body sodium while ADH (water excretion) and thirst (water intake) regulates total body water.
Hyponatremia is a failure of the regulation of:
Hyponatremia is a failure of the regulation of:
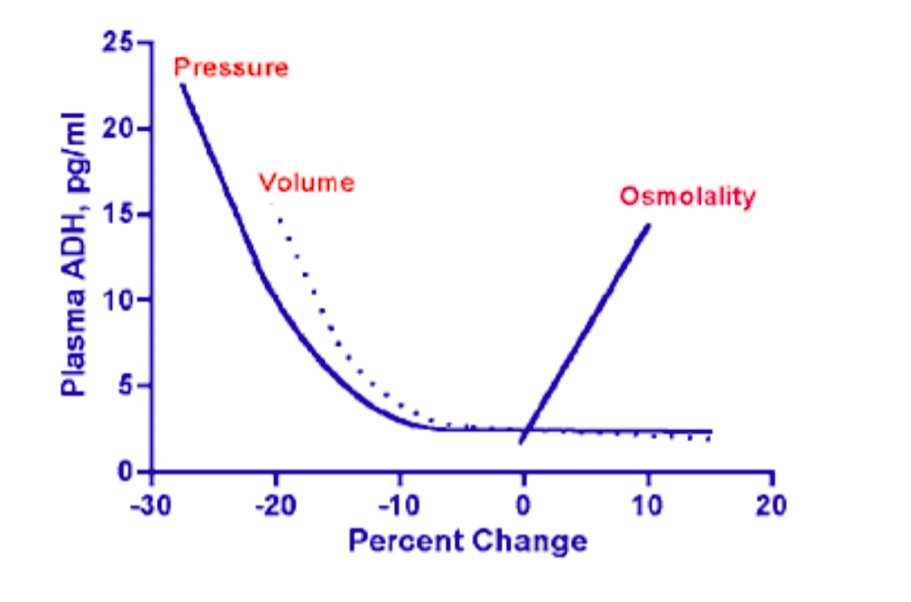
Though the two systems are independent there is some cross-over. When people get profound drops in perfusion ADH will be up regulated. This usually requires at least a 10-15% drop in perfusion. 
The drop in perfusion can come from good old volume depletion or from decreased blood pressure regardless of volume (high total body sodium). The later includes the three great edematous states:
1. Nephrotic syndrome
2. Heart failure
3. Cirrhosis
1. Nephrotic syndrome
2. Heart failure
3. Cirrhosis

The release of ADH (aka vasopressin) triggers V1 receptors causing vasoconstriction improving perfusion. The ADH also binds V2 receptors causing the kidney to reabsorb excess water diluting the sodium.
It is useful to group volume depletion and and the edematous states together because the kidney behaves similarly in all of them, that is the kidney will be sodium avid and absorb as much sodium as possible. Urine sodium will be low.
Any additional sodium in the form of 0.9% NaCl or salt tablets will help restore normal volume in people that are volume depleted and contribute to further edema in patients with CHF/Nephrotic syndrome/Cirrhosis.
Students often look at these cases and are puzzled why the patient has hyponatremia if the kidney is retaining sodium. The answer is:
Restoring volume in volume depleted people will suppress this perfusion stimulated release of ADH and they will then spontaneously diuresis the excess water and correct their hyponatremia. Giving salt tablets to people with volume deficiency will help correct their hyponatremia.
Giving three 1 gram salt tablets a day is equivalent to how much 0.9% normal saline?
Molecular weight of sodium chloride is 58.4
so 1 gram is 17 mmol (1 g /58.4 g/mol = 0.017 moles * 1000 mmol/mol)
So 1g tid is 51 mmol of Na and 51 mmol of Cl.
51 is a third of the 154 mmol per liter of 0.9% saline
so 1 gram is 17 mmol (1 g /58.4 g/mol = 0.017 moles * 1000 mmol/mol)
So 1g tid is 51 mmol of Na and 51 mmol of Cl.
51 is a third of the 154 mmol per liter of 0.9% saline
But giving salt tablets to people with heart failure, nephrotic syndrome, or cirrhosis is:
These patients are not in sodium balance and already are sodium overloaded (hence the edema) giving them salt tablets or normal saline or hypertonic saline will increase the edema (it may improve the sodium, but at the expense of the overall clinical status of the patient).
What about patients with 𝙏𝙚𝙖 𝙖𝙣𝙙 𝙏𝙤𝙖𝙨𝙩 𝙎𝙮𝙣𝙙𝙧𝙤𝙢𝙚. This is an unusual form of hyponatremia.
Normally urine volume roughly matches water intake, that is what ADH does:
Increased water intake =>lowers serum osmolality => suppresses ADH => Increases urine output
Increased water intake =>lowers serum osmolality => suppresses ADH => Increases urine output
Normally urine volume roughly matches water intake, that is what ADH does:
Decreased water intake => increases serum osmolality => stimulates ADH => decreases urine output
Decreased water intake => increases serum osmolality => stimulates ADH => decreases urine output
ADH doesn’t change the amount of solute in the urine, it just changes the water content of urine.
Lots of ADH, means just a little water and concentrated urine
Suppressed ADH means a lot of water and dilute urine
Lots of ADH, means just a little water and concentrated urine
Suppressed ADH means a lot of water and dilute urine
Urine osmolality can vary from 50 to 1,200 mOsm/Kg H2O. Normal osmolar intake is 10 mOsm/Kg so about 600 for a 60kg adult.
With 600 mOsm consumed the most urine a person could make is:
With 600 mOsm consumed the most urine a person could make is:
With 600 mOsm solute load the minimum amount of urine is:
To defend against hyponatremia suppressing ADH ⬆️ urine output and clears excess water. However, the minimum urine osm is 50 mOsm/Kg, so if a patient has an unusually low solute diet urine output may be limited.
What’s the max urine output for a patient eating 100 mOsm a day?
What’s the max urine output for a patient eating 100 mOsm a day?
So a low osmole or low solute diet will limit a person’s urine output even with maximally suppressed ADH. What does this diet look like? Carbs…nothing but carbs.

What about alcohol?
All carbohydrates.
No solute.
(please ignore the hgh protein beer in the corner) foodandwine.com/blogs/new-high…
All carbohydrates.
No solute.
(please ignore the hgh protein beer in the corner) foodandwine.com/blogs/new-high…
Carbs are metabolized to CO2 and water. You exhale CO2 and water is a solvent, not a solute. Fat is also metabolized to CO2 and water. If you want solute you need proteins and electrolytes. Protein is converted to urea & is excreted by the kidney with Na, K, Mg, Ca, Cl, PO4, etc
So how do you treat this lack of osmolar load? Ideally you fix the poor patient’s diet. Get them to increase the protein content fo their diet. More easily you can just give them salt. A liter of saline has enough solute for a patient with maximally dilute urine to make 6 liters.
solute load of one liter of 0.9% saline: 308 divided by maximally dilute urine at 50 mOsm/KgH2O = 6 liters of dilute urine
So 𝙩𝙚𝙖 𝙖𝙣𝙙 𝙩𝙤𝙖𝙨𝙩 𝙨𝙮𝙣𝙙𝙧𝙤𝙢𝙚, when it occurs is usually magically corrected in the ER when they give a liter of saline for dehydration that everyone with hyponatremia gets in the ER.
So add Tea and Toast to volume depletion as diseases that respond favorably to salt tablets.
Next up is the 𝙨𝙮𝙣𝙙𝙧𝙤𝙢𝙚 𝙤𝙛 𝙞𝙣𝙖𝙥𝙥𝙧𝙤𝙥𝙧𝙞𝙖𝙩𝙚 𝘼𝘿𝙃, 𝙎𝙄𝘼𝘿𝙃. The key to understanding this diagnosis is that these patients are in sodium balance:
Sodium in = sodium out
Sodium in = sodium out
That is why they are clinically euvolemic. These patients are able to clear all of the sodium they eat and remain in sodium balance, but they are unable to dilute their urine. They have the ADH switch turned to maximum and someone broke off the switch and threw it away.
This becomes a problem since at maximum urine concentration, urine volume is at a minimum and it becomes very easy for people to drink more than they can pee. If they do this then….hyponatremia.
Their urine concentration is fixed and set to maximum. They drink a lot of water they drink a little bit of water, none of these things affect their urine volume. The only way to change urine volume is by increasing the solute load.
Since sodium in = sodium out, and their urine concentration is fixed, if you increase sodium in, then you will increase sodium out and since the urine concentration is fixed, an increase in sodium means more urine out.
Increasing urine output makes it easier to get urine excretion to exceed water intake and that will get them headed in the right direction.
𝐓𝐡𝐢𝐬 𝐢𝐬 𝐧𝐨𝐭 𝐭𝐡𝐞 𝐰𝐡𝐨𝐥𝐞 𝐬𝐭𝐨𝐫𝐲 and the sodium content of the urine can make a difference. If the urine Na + urine K is greater than plasma sodium (or even approaches serum Na) then fluid restriction and salt tablets won’t save you.
So salt tablets in SIADH (if the urine Na + urine K < serum Na) increase the urine output and make it easier for patients to be in negative balance for water slowly correct or maintain their serum sodium.
And that’s it. Use salt tablets in:
1. Tea and Toast syndrome (or its alcoholic uncle: Beer Drinkers Potomania)
2. Volume depletion
3. SIADH
Otherwise, they don’t work and can actually make patients sicker.
/fin
1. Tea and Toast syndrome (or its alcoholic uncle: Beer Drinkers Potomania)
2. Volume depletion
3. SIADH
Otherwise, they don’t work and can actually make patients sicker.
/fin












