,
10 tweets,
4 min read
Read on Twitter
1/How your health information is sold and turned into ‘risk scores’ - from @politico ...Let me share a couple insights from using a risk tool paid for by US taxpayers politico.com/story/2019/02/…
2/First, risk scores of high quality use all health information, as VA studies show risk for OD/suicide reflects (a) medical + mental + prior substance use, & (b) # of co-prescribed sedating mess that are crucial. Actual #opioid dose, formulation are relevant, but less so 
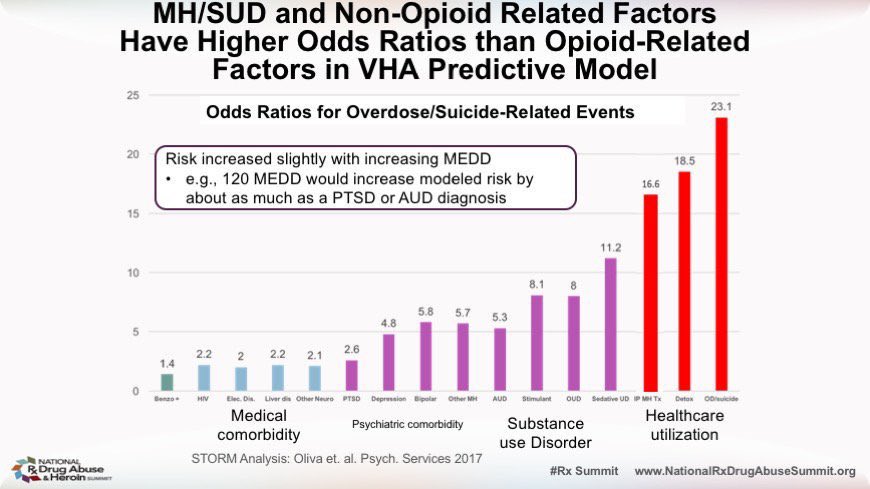
3/Second, in studies & our biweekly opioid risk mitigation meetings we find most people at risk are at low opioid dose, often not chronic recipients at all, but have significant mental health care needs. We see this again and again.
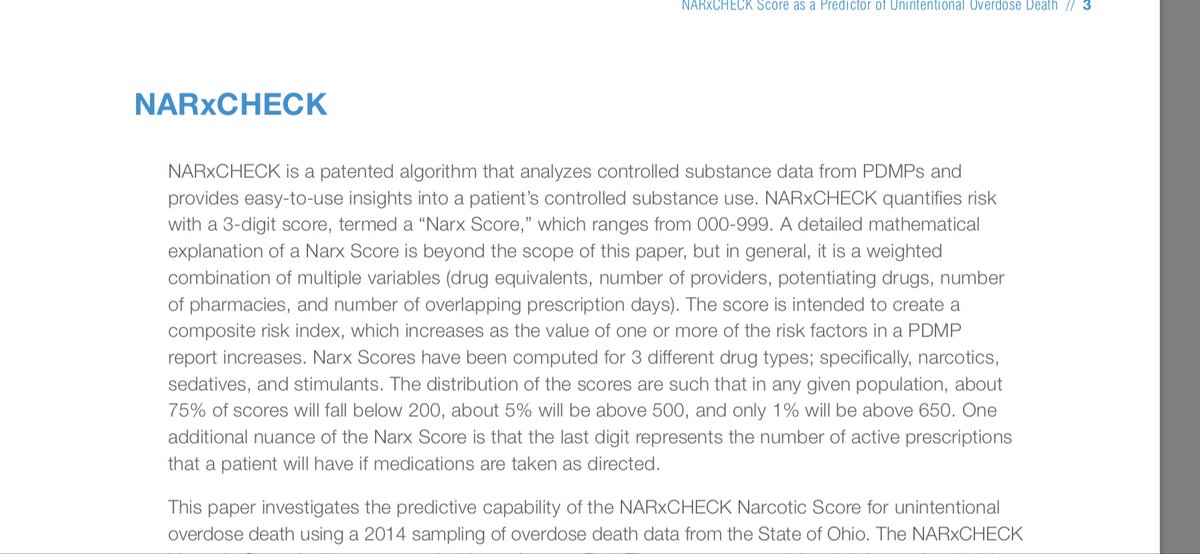
4/note that NarxCheck- bundled with PDMP as sold by @appriss relies solely on Prescription data: it lacks nearly _all_ statistically valid clinical indicators of risk in opioid-receiving patients, but still describes its indicators “red flag$” pmp.pharmacy.state.mn.us/assets/files/N…
5/Fourth, no one has proven what actual clinical care is most protective of patients on opioids who receive a high score. While @DeptVetAffairs has stood up multidisciplinary teams to craft protective care plans, uniquely, I don’t think any commercial entity has tried
6/Fifth- thus, the “risk score” hasn’t been shown to protect patients. Using it in good faith to deliver more care, protectively, seems right to me. But in the current environment, they are more likely to be used to flag patients as liabilities.
8/any insurer or payer or quality arbiter or quality agency that wishes to discuss setting up & paying for care that really protects patients? Let’s talk (no charge). We can’t protect patients when we buy and sell systems that make them into liabilities.
9/Re: accuracy problems: I have seen Narxcare designates a patient as risk for “multiple prescribers” when docs in a shared practice cover each others’ patients, with all operating under carefully designed opioid protocols &clear supervision. Should inaccurate data be profitable?
10/ as clinical matter - mitigating risk in patients with multiple health conditions + medications requires a clinical team, including mental health and pharmacy care. You want safety? I think care relationships with caring expert providers are more likely to deliver.