.@StanfordPath Saturday!
📝 58 YO female with elevated CA125 with colonic mass
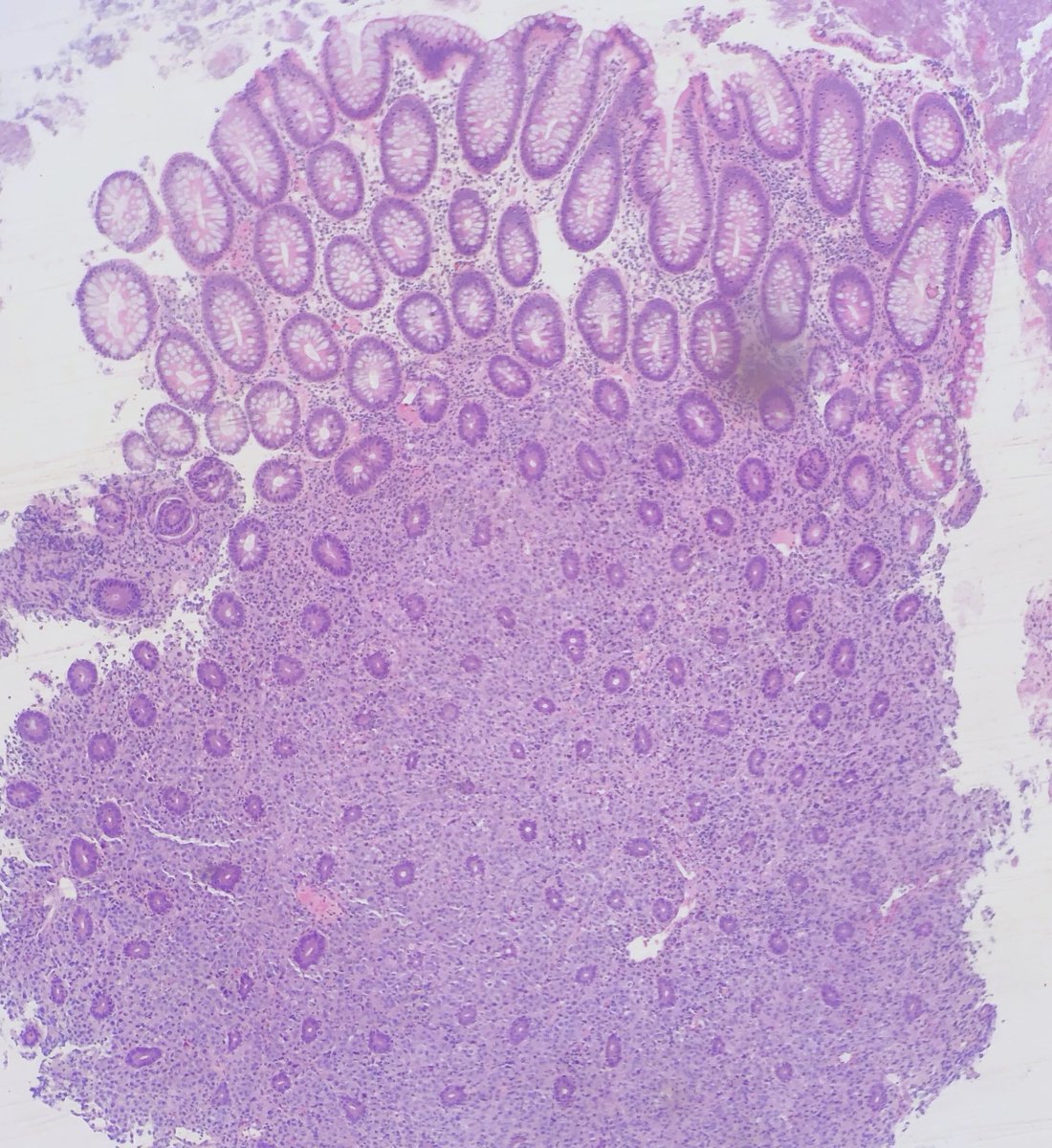
🔬 Poorly differentiated epithelioid malignancy intercalating between colonic lamina propria
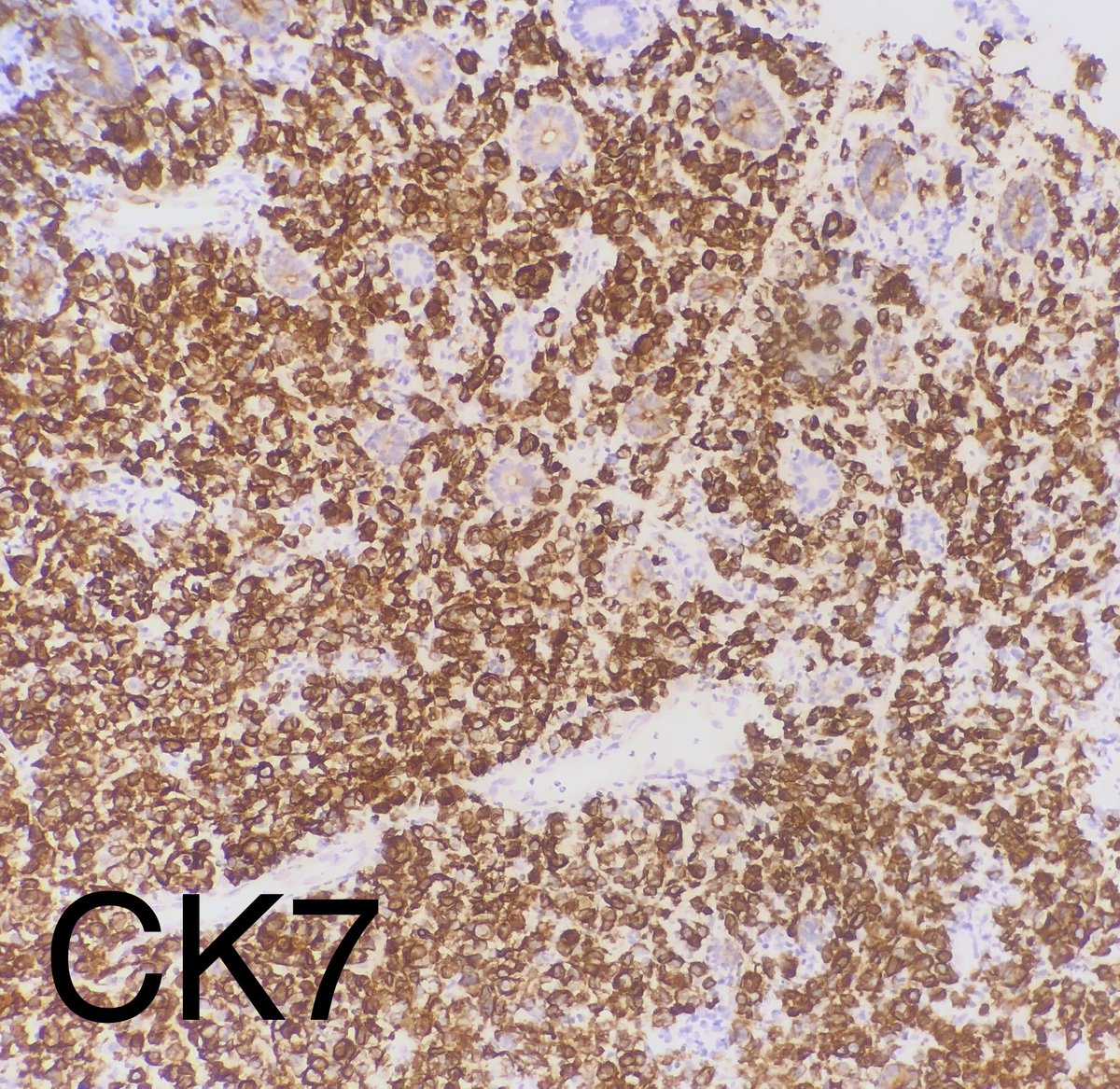
IHC: CK7+, CK20-, CDX2-, PAX8-, GATA3-, S100-, synapto-
#stanfordpathsaturday #MedEd #pathologytwitter
📝 58 YO female with elevated CA125 with colonic mass
🔬 Poorly differentiated epithelioid malignancy intercalating between colonic lamina propria
IHC: CK7+, CK20-, CDX2-, PAX8-, GATA3-, S100-, synapto-
#stanfordpathsaturday #MedEd #pathologytwitter
This one stumped us at first...is this primary, is it a met? We considered breast, gyn, gastric, and melanoma. We talked to the the gastroenterologist who insisted that colonoscopy was suggestive of primary colon cancer. So we proceeded to perform MSI, shown below.




So we have loss of mismatch repair proteins MLH1 and PSM2. We proceeded to molecular for BRAF and this lesion does have a BRAF V600E mutation. 🧬
Therefore given the poorly differentiated morphology, the clinical impression, and molecular findings, we diagnosed this as colonic adenocarcinoma, medullary type.
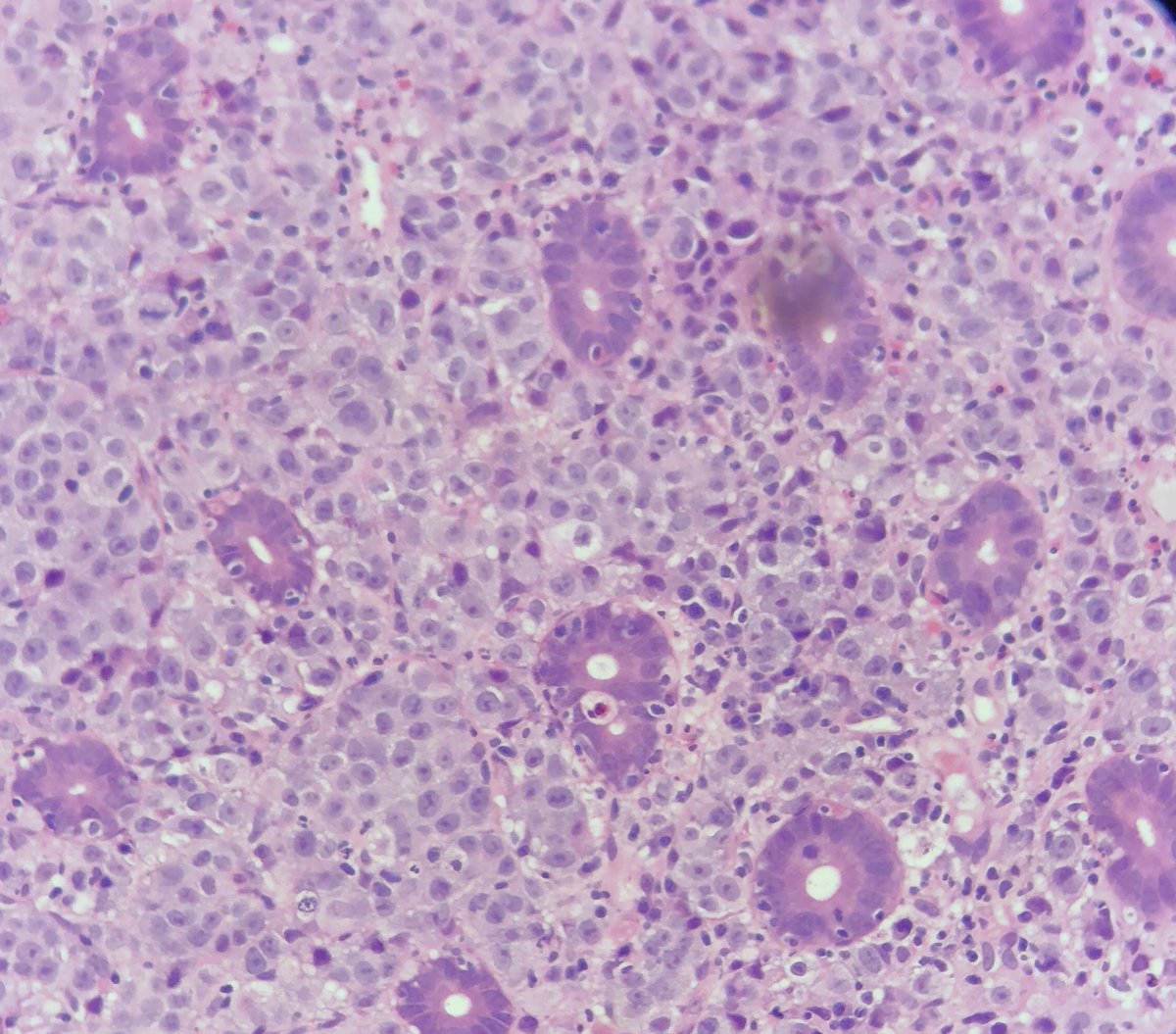
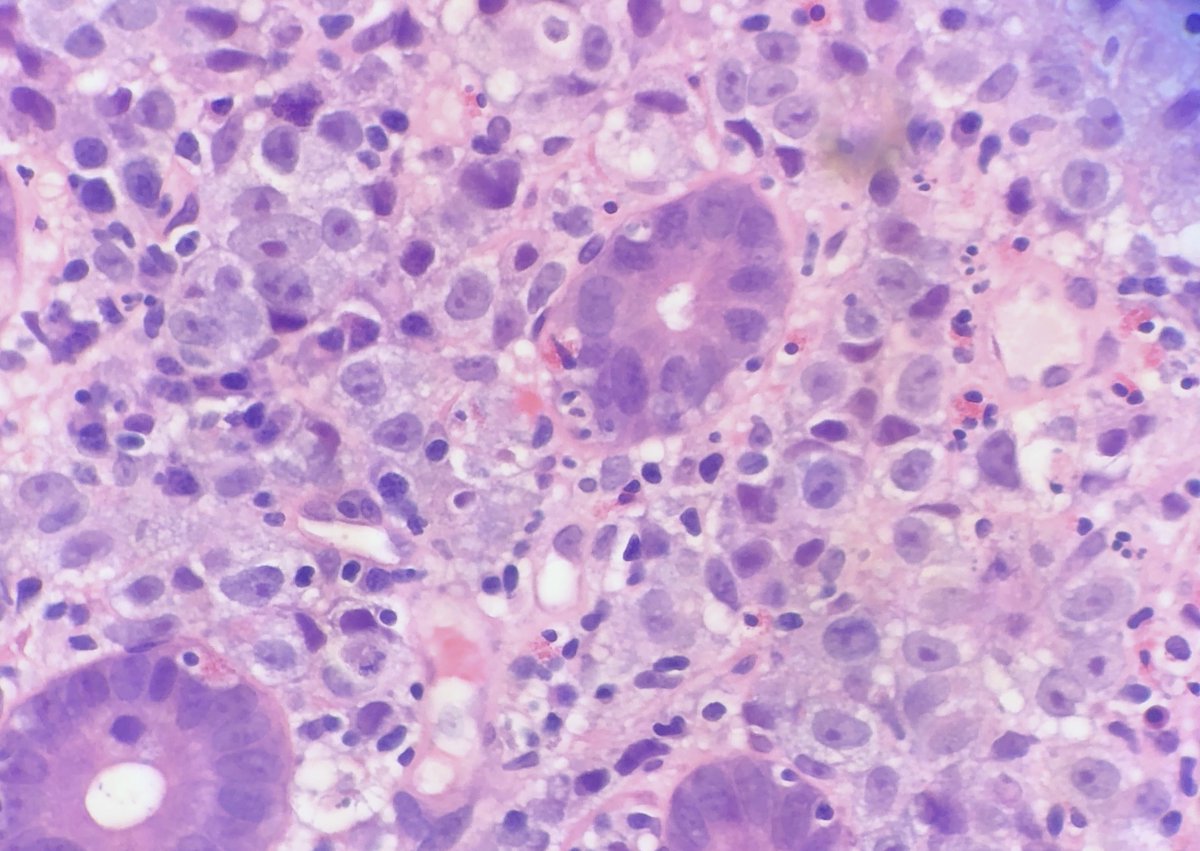
🔬Medullary type CRC shows poorly differentiated carcinoma cells usually arranged in sheets or trabeculae and do not form glands. They are medium in size with vesicular chromatin and often prominent nucleoli.
They often have tumor infiltrating lymphocytes (TILs!) along with a Crohn's like response. These features are often seen in mismatch repair CRC of any architectural type. So it's not surprising they often have MSI.
🧬Although they can be associated with Lynch, many times they are sporadic, hence they will usually harbor a BRAF V600E mutation.
IHC is variable. Many show loss of traditional CRC markers like CK20 and CDX2, which can be scary and can send you down the wrong path. In this case, MMR protein IHC can be used as a diagnostic tool in addition to its usual prognostic/genetic counseling screen.
Ddx includes mets (lobular breast, poorly diff carcinoma, melanoma, poorly differentiated gastric), as well as undifferentiated carcinoma and neuroendocrine tumors/carcinoma.
Demographically, our case fit the textbook. They usually are right sided (ours was found in the ascending colon) and are more common in women.
Although they look poorly differentiated, Medullary type CRC typically carries a good prognosis. Probably because of the MMR protein deficiency leads to subsequent immune response to cancer cells.
Take home point: While poorly differentiated malignancies in the colon should make you consider a metastasis, don't be afraid to throw on MMR IHC because it can be used to help in the diagnosis of medullary type primary CRC, not just the usual molecular/genetic counseling screen.
Alrighty...back to my hotseat cases here @StanfordPath. Have a good weekend! #stanfordpathsaturday