1/ Welcome to the next installment of @NEJM #CPS summaries!
For full case: bit.ly/2SWTDiq
@MedTweetorials
40yo F w/ hx of treated immature teratoma & HBV infection p/w chronic, progressive diffuse pain and weight loss
Me when I get to share clinical pearls 👇🏾
For full case: bit.ly/2SWTDiq
@MedTweetorials
40yo F w/ hx of treated immature teratoma & HBV infection p/w chronic, progressive diffuse pain and weight loss
Me when I get to share clinical pearls 👇🏾
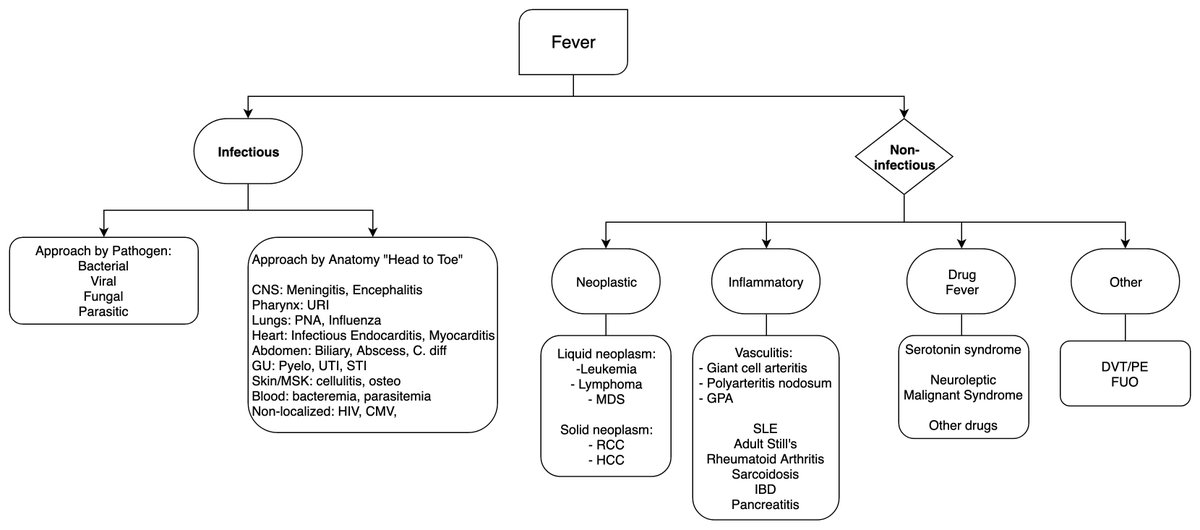
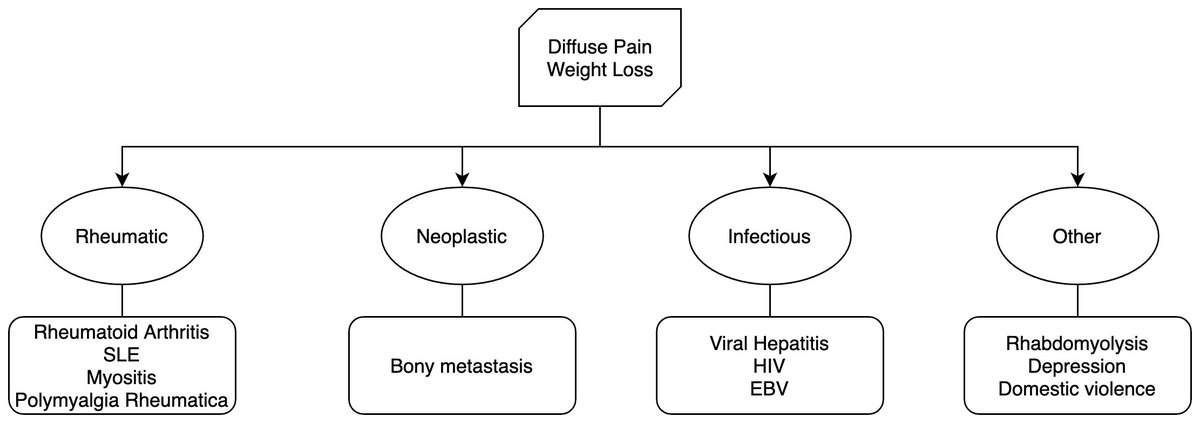
2/ 🌟Initial DDx 🌟
#medstudenttwitter: I often find it tempting to jump straight into listing possible Dx.
Often have to remind myself to be systematic. For this patient:
Up next: how does the PMHx ("background") affect our analysis of this presentation ("foreground")
#medstudenttwitter: I often find it tempting to jump straight into listing possible Dx.
Often have to remind myself to be systematic. For this patient:
Up next: how does the PMHx ("background") affect our analysis of this presentation ("foreground")
3/ 📚 History:
Teratoma: tx w/ 4 cycles of bleomycin, etoposide & cisplatin → TAH-BSO
HBV: tx w/ tenofovir
Immigrated from Vietnam 20 years ago
🧠Clinical reasoning: when evaluating "background" I ask myself 3 questions 👇🏾
Teratoma: tx w/ 4 cycles of bleomycin, etoposide & cisplatin → TAH-BSO
HBV: tx w/ tenofovir
Immigrated from Vietnam 20 years ago
🧠Clinical reasoning: when evaluating "background" I ask myself 3 questions 👇🏾

4/
🔍 Exam
• normal vitals
• cachectic, ill-appearing (BMI 16.2)
• diffuse tenderness on palpation of the abdomen; pos Murphy's sign.
🧪Labs
• K 2.7
• Bicarb 15
• mild amylase/lipase⬆️
• AP 242 U/L
• LFTs normal
• Cr 0.72 mg/dL
🔍 Exam
• normal vitals
• cachectic, ill-appearing (BMI 16.2)
• diffuse tenderness on palpation of the abdomen; pos Murphy's sign.
🧪Labs
• K 2.7
• Bicarb 15
• mild amylase/lipase⬆️
• AP 242 U/L
• LFTs normal
• Cr 0.72 mg/dL
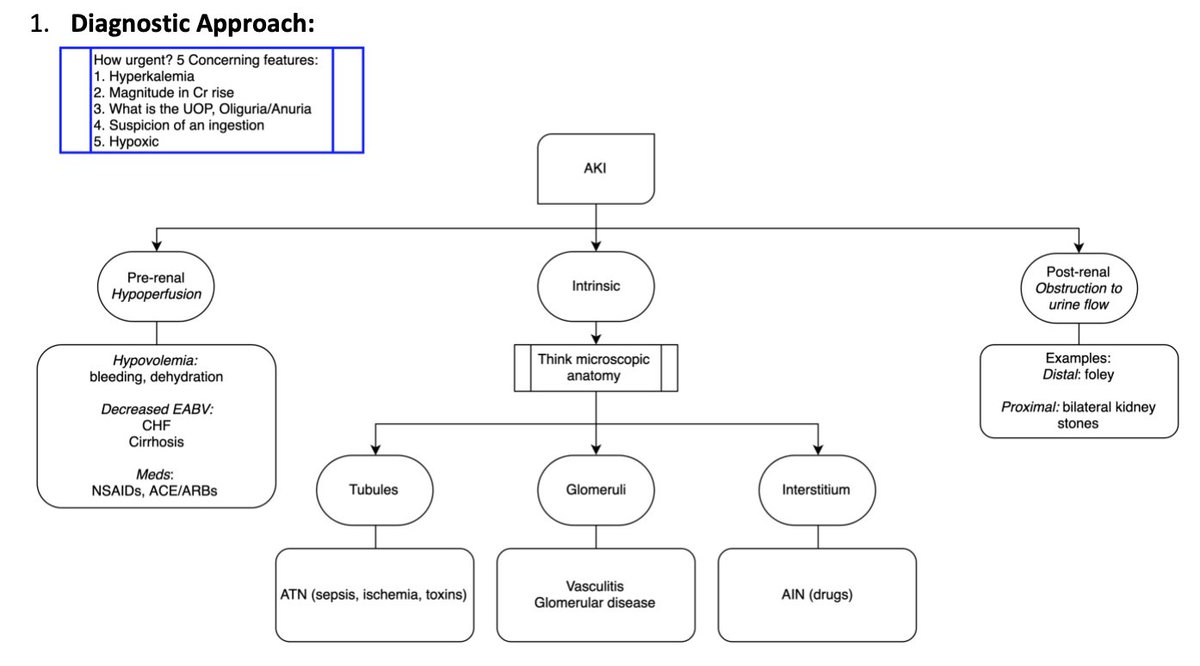
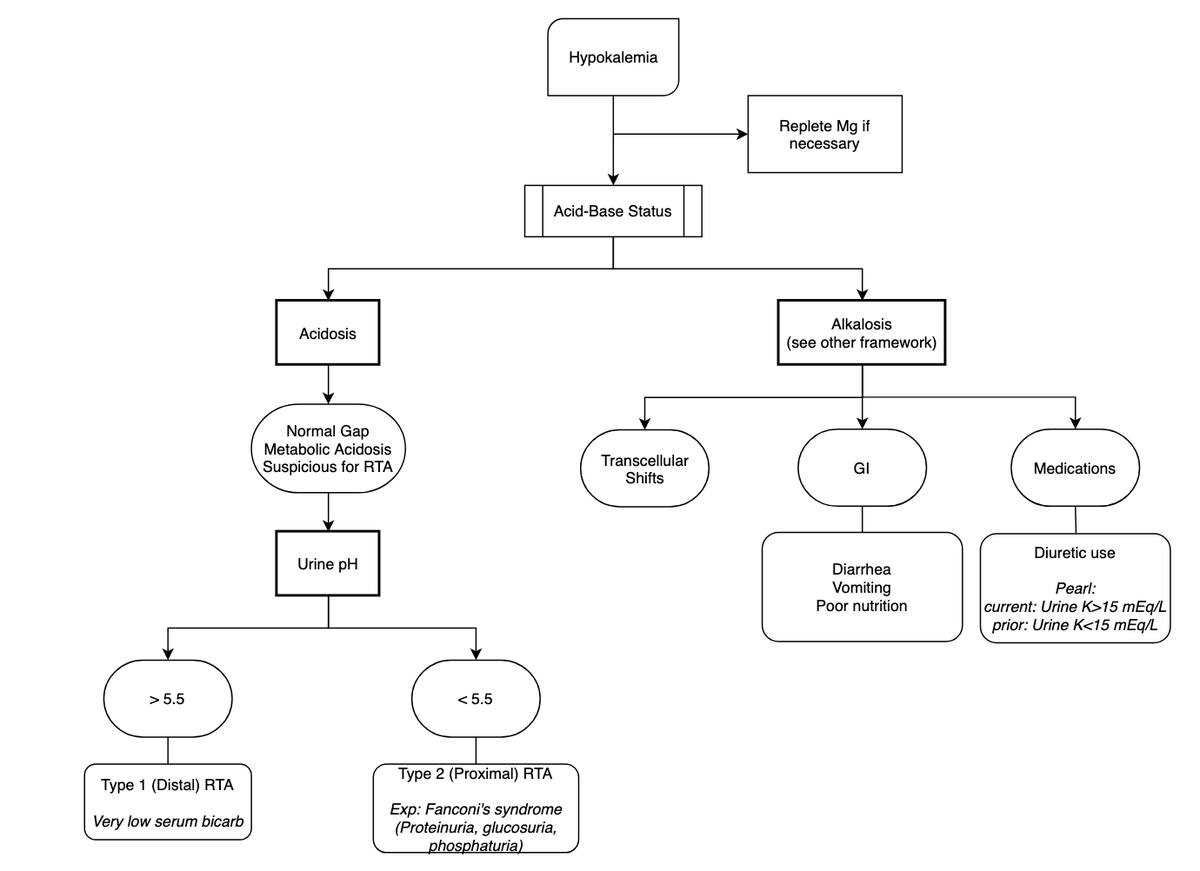
5/ Let's practice integrating all this info!
🤔Hypokalemia → probably renal/GI losses + low bicarb → RTA vs. diarrhea?
Cr is "normal" but muscle mass low → localizing kidney injury? 👀
🧐Alk Phos is high. Key question: biliary or bony origin?
med.upenn.edu/frameworks/hyp…
🤔Hypokalemia → probably renal/GI losses + low bicarb → RTA vs. diarrhea?
Cr is "normal" but muscle mass low → localizing kidney injury? 👀
🧐Alk Phos is high. Key question: biliary or bony origin?
med.upenn.edu/frameworks/hyp…
6/
RUQ U/S w/o evidence of cholecystitis
CT-Abd: post-op changes
Bone scan: multiple abnormal areas with increased tracer uptake + osteopenia
MRI: healing, nondisplaced fracture of the R. femoral neck + enhancing lesion in the distal L humerus w/ surrounding mild edema
RUQ U/S w/o evidence of cholecystitis
CT-Abd: post-op changes
Bone scan: multiple abnormal areas with increased tracer uptake + osteopenia
MRI: healing, nondisplaced fracture of the R. femoral neck + enhancing lesion in the distal L humerus w/ surrounding mild edema

7/ ❤️ how @CPSolvers normalize "I don't know"
🧠my cognitive bias: saw bone scan & jumped to conclusion: metastatic ca. DDx is way broader!
• Osteomalacia
• Paget's dz
Not multifocal:
• osteomyelitis
• avascular necrosis
• bone infarcts
Schema 👇🏾
clinicalproblemsolving.com/dx-schema-bone…
🧠my cognitive bias: saw bone scan & jumped to conclusion: metastatic ca. DDx is way broader!
• Osteomalacia
• Paget's dz
Not multifocal:
• osteomyelitis
• avascular necrosis
• bone infarcts
Schema 👇🏾
clinicalproblemsolving.com/dx-schema-bone…
8/
CA-125 & AFP normal
Phosphate: 0.5
Calcium: 8.3
Normal Vit. D & iPTH
bone-specific AlkPhosh was 57.1
🌟Updated DDx 🌟
Hypophos usually 2/2 renal losses w/ ⬆️ PTH or FGF-23
+ hypokalemia & low bicarb →
Think Fanconi syndrome
CA-125 & AFP normal
Phosphate: 0.5
Calcium: 8.3
Normal Vit. D & iPTH
bone-specific AlkPhosh was 57.1
🌟Updated DDx 🌟
Hypophos usually 2/2 renal losses w/ ⬆️ PTH or FGF-23
+ hypokalemia & low bicarb →
Think Fanconi syndrome
9/
fractional excretion of phosphate: 37.9%
24-hour: 367 mg of phosphate
Normal FGF, S/UPEP
UA: 2+ glucose, 1+ ketones, 1+ blood, and 2+ protein; pH was 7.0
Final diagnosis:
🚨 proximal renal tubular dysfunction (renal Fanconi's syndrome) 2/2 tenofovir 🚨
fractional excretion of phosphate: 37.9%
24-hour: 367 mg of phosphate
Normal FGF, S/UPEP
UA: 2+ glucose, 1+ ketones, 1+ blood, and 2+ protein; pH was 7.0
Final diagnosis:
🚨 proximal renal tubular dysfunction (renal Fanconi's syndrome) 2/2 tenofovir 🚨
10/ Summary+Pearls
🧪clinical manifestations of hypophosphatemia rarely apparent until levels fall below 1 mg/dL
2° causes of prox RTA dysfunction: myeloma, amyloidosis, Sjögren's
💊 Med causes: acetazolamide, topiramate, ifosfamide, tenofovir + heavy metals
Thx for joining!
🧪clinical manifestations of hypophosphatemia rarely apparent until levels fall below 1 mg/dL
2° causes of prox RTA dysfunction: myeloma, amyloidosis, Sjögren's
💊 Med causes: acetazolamide, topiramate, ifosfamide, tenofovir + heavy metals
Thx for joining!