Ever found DVT POCUS challenging? We do.
Here is a #Tweetorial on #POCUS for Lower Extremity DVT assessment. Let’s walk through a case and discuss common questions that arise.
50s f no PMH presenting to the ED on a Friday evening with right leg swelling and redness...
1/
Here is a #Tweetorial on #POCUS for Lower Extremity DVT assessment. Let’s walk through a case and discuss common questions that arise.
50s f no PMH presenting to the ED on a Friday evening with right leg swelling and redness...
1/
History/exam/labs:
No travel, surgeries, immobilization. No dyspnea, CP. No meds. No FH of VTE. no tobacco.
HR 88 SpO2 98% RA BP 160/90 T 37.
Exam unremarkable other than 2+ LE edema erythema and tenderness from right ankle to knee.
CBC/BMP/coags normal
2/
No travel, surgeries, immobilization. No dyspnea, CP. No meds. No FH of VTE. no tobacco.
HR 88 SpO2 98% RA BP 160/90 T 37.
Exam unremarkable other than 2+ LE edema erythema and tenderness from right ankle to knee.
CBC/BMP/coags normal
2/
Wells-DVT score 1 (for pitting edema confined to symptomatic leg), with a moderate pre-test probability for DVT.
It is Saturday. Formal vascular study (FVS) is not available until Monday. D-dimer is considered. Would you check D-dimer in this case? (poll)
3/
It is Saturday. Formal vascular study (FVS) is not available until Monday. D-dimer is considered. Would you check D-dimer in this case? (poll)
3/
Won't go much into D-dimer.
General rule - important to consider plan for each possible outcome, based on pre-test probability (and possible non-DVT causes of D-dimer elev). If the plan would differ and resource use of lab test < imaging test, would be high value to check.
4/
General rule - important to consider plan for each possible outcome, based on pre-test probability (and possible non-DVT causes of D-dimer elev). If the plan would differ and resource use of lab test < imaging test, would be high value to check.
4/




Here, pre-test prob is moderate. D-dimer up (1.2). Formal vascular study will be delayed for 2 days. No cardiopulmonary disease and no signs/symptoms of PE. Minimal bleeding risk. Pt agreeable to whatever recommended.
In the absence of POCUS, what would you recommend (poll)?
5/
In the absence of POCUS, what would you recommend (poll)?
5/
See algorithm here for initial approach, adapted from CHEST guidelines. No mention of POCUS in this algorithm though.
6/
6/

So in this thread, we consider how POCUS DVT study fits in...
Here is a proposed table, with a consideration of non-POCUS management plan, and how it may be influenced by POCUS.
Interestingly, POCUS *may* influence management approach in all scenarios, depending on result.
7/
Here is a proposed table, with a consideration of non-POCUS management plan, and how it may be influenced by POCUS.
Interestingly, POCUS *may* influence management approach in all scenarios, depending on result.
7/

So we will do POCUS DVT study. But what exactly is that?
POCUS DVT study uses proximal compression US (CUS) (and possibly other adjuncts) by the treating clinician. As w all POCUS, heterogeneity in operating characteristics depending on:
-Protocol
-Operator
-QA system
etc.
8/
POCUS DVT study uses proximal compression US (CUS) (and possibly other adjuncts) by the treating clinician. As w all POCUS, heterogeneity in operating characteristics depending on:
-Protocol
-Operator
-QA system
etc.
8/
Let's talk a bit about protocols.
Which POCUS DVT study protocol do you normally use/recommend? (poll)
2 Point Compression Ultrasound (2PCUS)
3 Point compression Ultrasound (3PCUS)
Extended Compression Ultrasound (ECUS)
Other
9/
Which POCUS DVT study protocol do you normally use/recommend? (poll)
2 Point Compression Ultrasound (2PCUS)
3 Point compression Ultrasound (3PCUS)
Extended Compression Ultrasound (ECUS)
Other
9/
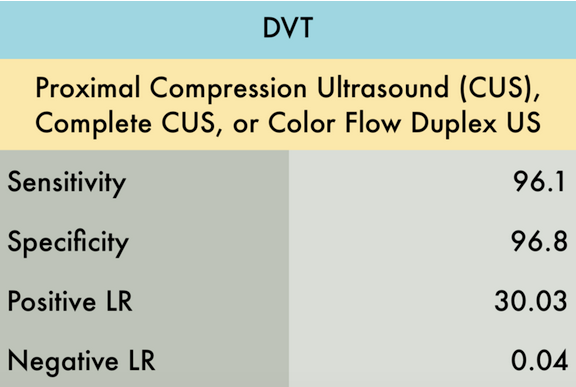
There is literature on all of these with heterogeneous results. See below, including:
-Great illustrations/data from @thepocusatlas and @ultrasoundgel
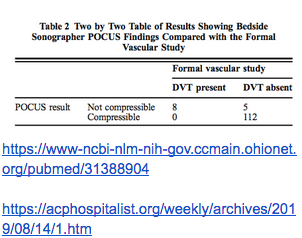
-The (dare-I-say?) landmark #IMPOCUS study #HOCUSPOCUS on hospitalist DVT POCUS, which warrants a journal club of its own
10/
-Great illustrations/data from @thepocusatlas and @ultrasoundgel
-The (dare-I-say?) landmark #IMPOCUS study #HOCUSPOCUS on hospitalist DVT POCUS, which warrants a journal club of its own
10/
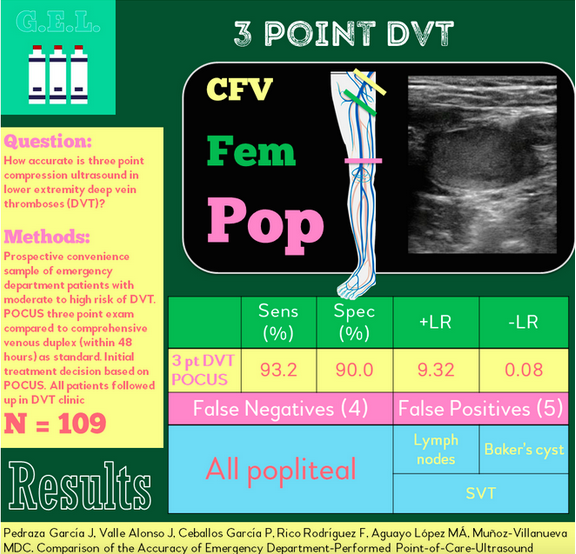
Opinion/Conclusion: sensitivity best with extended compression ultrasound, with minimal additional time. Best to compress q2-3 cm from inguinal ligament to adductor canal, and entire popliteal fossa to trifurcation.
See below for anatomy review/protocol descriptions
11/
See below for anatomy review/protocol descriptions
11/



False positives on POCUS DVT study (important to be aware of)
-Lymph node
-Baker cyst
-Superficial thrombosis
-Incomplete compression (ex: inadequate pressor, soft tissue limitations to compression). Visualizing compression of artery should indicate adequate compression.
12/
-Lymph node
-Baker cyst
-Superficial thrombosis
-Incomplete compression (ex: inadequate pressor, soft tissue limitations to compression). Visualizing compression of artery should indicate adequate compression.
12/




Worth noting the possibility of true pos POCUS DVT study, with subsequent neg “formal vascular study” (FVS), either due to false neg FVS or interval dissolution/embolization.
Emphasizes importance of saving POCUS images (and report) for documentation/ verification.
13/
Emphasizes importance of saving POCUS images (and report) for documentation/ verification.
13/
14/
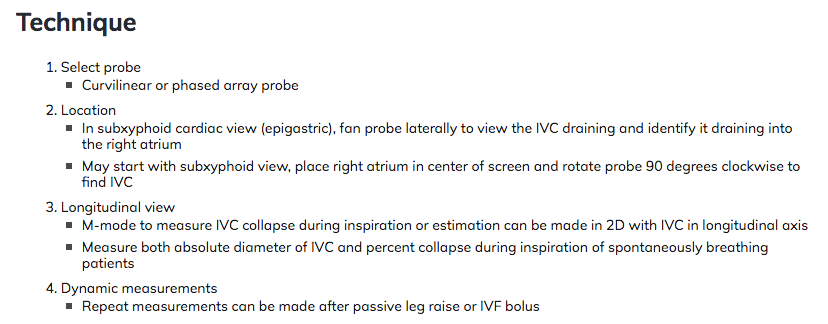
Image acquisition tips
1) Compress --> clip --> release (rather than clip --> compress --> release). This helps keep vessels centered throughout clip.
2) Avoid using color flow during compression - probe movement will cause color to obscure visualization.
Image acquisition tips
1) Compress --> clip --> release (rather than clip --> compress --> release). This helps keep vessels centered throughout clip.
2) Avoid using color flow during compression - probe movement will cause color to obscure visualization.
Back to the case! Here are the images
First: L CFV at saphenofemoral junction (SFJ)
15/
First: L CFV at saphenofemoral junction (SFJ)
15/
L CFV (inadequate compression)
16/
16/
L CFV and DFV (choppy image, but demonstrates full compression of veins)
17/
17/
left pop vein (less depth would improve image). more left images would have been preferred
18/
18/
R CFV at SFJ
19/
19/
R CFV in long axis with color flow
20/
20/
R CFV in short axis with color (no compression applied)
21/
21/
RFV with compression
22/
22/
R femoral vein and deep femoral vein with compression applied
23/
23/
long clip of attempted extended compression of right thigh veins
24/
24/
right pop vein
25/
25/
And back to the original question… what management would you choose (poll)
26/
26/
Impression
Evidence of DVT seen in the right leg from popliteal to common femoral vein
Indeterminate exam of left leg (cannot exclude popliteal vein thrombus)
27/
Evidence of DVT seen in the right leg from popliteal to common femoral vein
Indeterminate exam of left leg (cannot exclude popliteal vein thrombus)
27/
In this case, POCUS was found to be positive for DVT in a pt with moderate pretest probability, expediting diagnosis and earlier management, and aiding in triage decisions. If study was negative, confirmatory study would have still been obtained to confirm.
28/
28/
Potential pitfall of making wrong decision based on limited images (ex: left PV may have been called a DVT, which could have prompted AC). Maybe “indeterminate” should be a reportable result?
OR finding a DVT on POCUS, but not acting on it, with subsequent propagation to PE.
29/
OR finding a DVT on POCUS, but not acting on it, with subsequent propagation to PE.
29/
Once 1 clot is found, would you continue to compress other nearby veins? (poll)
(No clear answer. Would argue yes, to evaluate extent of disease, same as FVS, but keep it to a minimum)
30/
(No clear answer. Would argue yes, to evaluate extent of disease, same as FVS, but keep it to a minimum)
30/
Summary
-before DVT POCUS, have a plan for possible outcomes
-Sens/spec varies, can be very good in some studies
-Extended CUS is probably most sensitive
-Compress, then clip
-False positives (LNs, baker, superficial, incomplete compression)
-Saving images is important
31/
-before DVT POCUS, have a plan for possible outcomes
-Sens/spec varies, can be very good in some studies
-Extended CUS is probably most sensitive
-Compress, then clip
-False positives (LNs, baker, superficial, incomplete compression)
-Saving images is important
31/
We welcome all additional thoughts/discussion related to this case or to DVT POCUS!
and check out 5 minute sono: 5minsono.com/dvt1/ for the top-notch description of the technique
and check out 5 minute sono: 5minsono.com/dvt1/ for the top-notch description of the technique
Very good point brought up here by @VascularSci: there is a role to waveform analysis, assessment for augmentation, etc...
We limited the scope of this thread to compression only, and there is evidence for that strategy, but there is more than just that!
We limited the scope of this thread to compression only, and there is evidence for that strategy, but there is more than just that!
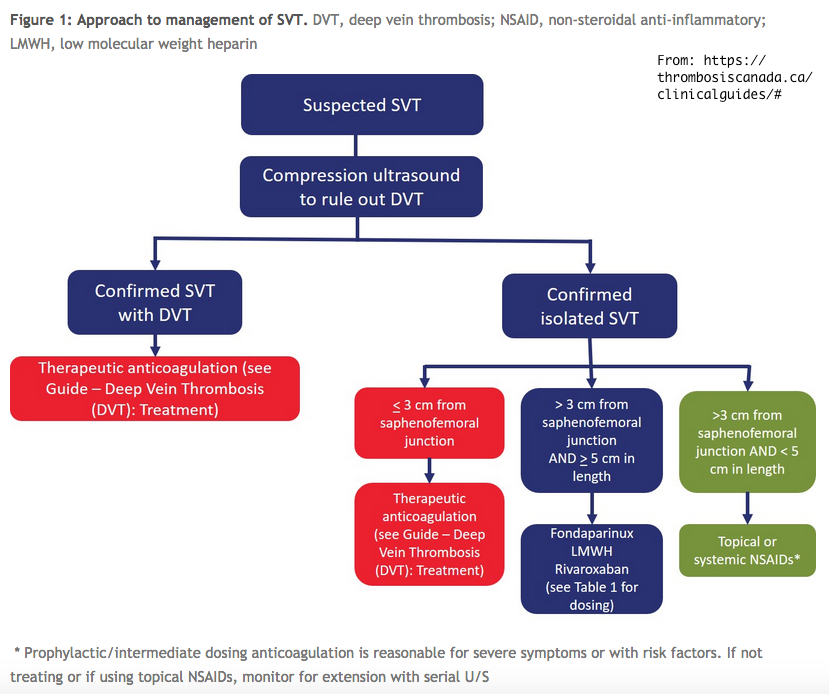
@VascularSci And a reminder of importance of superficial venous thrombosis (SVT) along with a great resource for how to manage those pesky superficial clots.
@VascularSci also will include this very recent article with a related discussion of POCUS DVT protocols
@VascularSci Bringing to main thread - makes sense as an answer to the question regarding whether to continue to examine once a clot is found.