2/
HPI:
well until 3 months ago. Since then, progressive fatigue, nausea, mild diffuse itching without rash. Few weeks of early satiety, poor PO intake, and now increasing abdominal girth. Last BM 3 days ago. No vomiting. Weight unchanged over 3 months. No fevers/chills.
HPI:
well until 3 months ago. Since then, progressive fatigue, nausea, mild diffuse itching without rash. Few weeks of early satiety, poor PO intake, and now increasing abdominal girth. Last BM 3 days ago. No vomiting. Weight unchanged over 3 months. No fevers/chills.
3/
No home meds. 2-3 etoh drinks per day (none for a few wks). Unable to work due to symptoms. Past 1-2 days he has become confused and unable to ambulate.
No home meds. 2-3 etoh drinks per day (none for a few wks). Unable to work due to symptoms. Past 1-2 days he has become confused and unable to ambulate.
4/
HR 95 BP 100/70 SpO2 100% RA RR 20 T 37
Thin, Lethargic.
A/O to person, place, moves all extremities. +asterixis.
Abd soft, NT, distended, ?fluid wave, +shifting dullness, no r/g.
2+ LE edema.
No spider angio, palmar erythema, caput med, or rash
HR 95 BP 100/70 SpO2 100% RA RR 20 T 37
Thin, Lethargic.
A/O to person, place, moves all extremities. +asterixis.
Abd soft, NT, distended, ?fluid wave, +shifting dullness, no r/g.
2+ LE edema.
No spider angio, palmar erythema, caput med, or rash
5/
WBC 6 Hb 10 PLT 70
Alb 2.6, prot 5.2 Bili 0.3 AST 14 ALT 18 Alk Phos 271 GGT 100
INR: 1.4
BMP: all normal
Due to concern for inability to safely swallow meds, narrow bore nasoenteric tube was placed.
Abd XR is shown
WBC 6 Hb 10 PLT 70
Alb 2.6, prot 5.2 Bili 0.3 AST 14 ALT 18 Alk Phos 271 GGT 100
INR: 1.4
BMP: all normal
Due to concern for inability to safely swallow meds, narrow bore nasoenteric tube was placed.
Abd XR is shown

6/
Any additional history questions?
DDx?
(poll) What is the most likely contributor to the abdominal distension?
A) Ascites
B) GI obstruction
C) Intraabdominal mass
D) 2 or more of the above
Any additional history questions?
DDx?
(poll) What is the most likely contributor to the abdominal distension?
A) Ascites
B) GI obstruction
C) Intraabdominal mass
D) 2 or more of the above
7/
(poll) You are admitting pt overnight. Without POCUS immediately available, what would be your next step?
A) CT A/P
B) Abd US, including liver vascular doppler
C) Request paracentesis
D) Large bore NG tube placement
(poll) You are admitting pt overnight. Without POCUS immediately available, what would be your next step?
A) CT A/P
B) Abd US, including liver vascular doppler
C) Request paracentesis
D) Large bore NG tube placement
8/
The clinician was thinking a CT scan may be helpful but more assessment was warranted. POCUS was used primarily to help determine extent of ascites and to guide decisions regarding paracentesis. The following images are obtained
First - sweeping LUQ/epigastric (longitudinal)
The clinician was thinking a CT scan may be helpful but more assessment was warranted. POCUS was used primarily to help determine extent of ascites and to guide decisions regarding paracentesis. The following images are obtained
First - sweeping LUQ/epigastric (longitudinal)
9/
LUQ/epigastric (longitudinal)
LUQ/epigastric (longitudinal)
10/
LUQ/epigastric transverse
LUQ/epigastric transverse
11/
Mid-epigastric transverse
Mid-epigastric transverse
12/
Sweeping midabd, transverse
Sweeping midabd, transverse
13/
Midabd, transverse
Midabd, transverse
14/
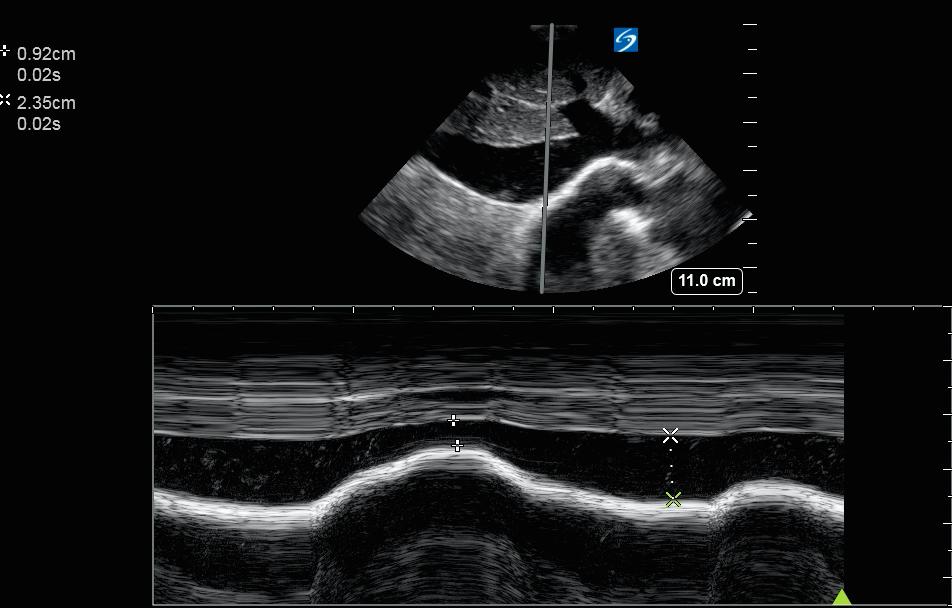
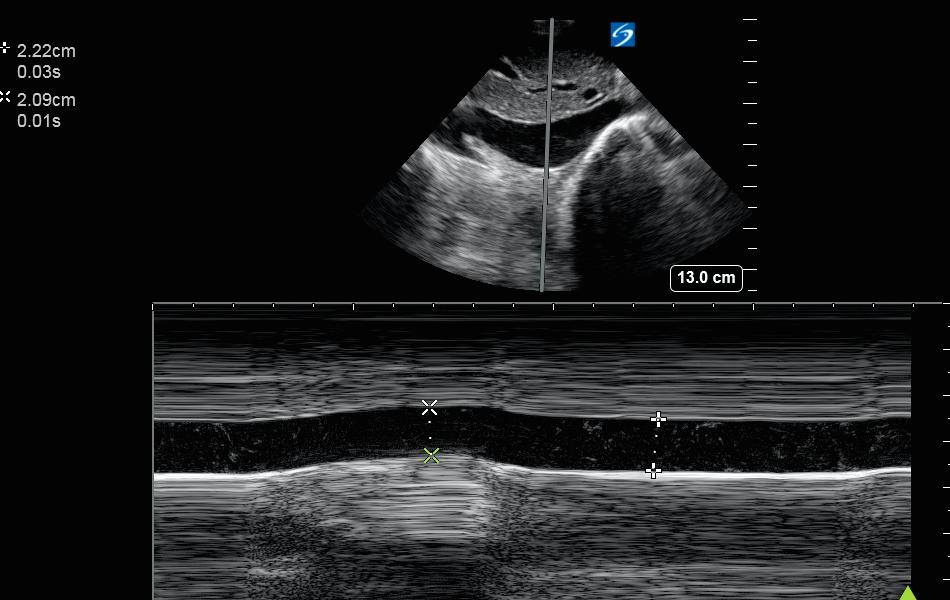
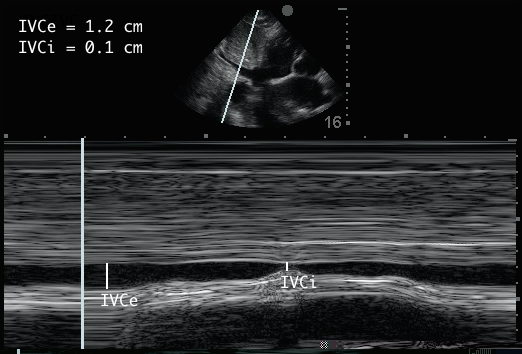
Still image of small bowel shown here, with measurement
Other views (liver, spleen, kidneys, bladder) not shown for brevity
Unable to locate large bowel
Cardiac: grossly normal LV systolic function, no pericardial effusion, no RV dilation
Still image of small bowel shown here, with measurement
Other views (liver, spleen, kidneys, bladder) not shown for brevity
Unable to locate large bowel
Cardiac: grossly normal LV systolic function, no pericardial effusion, no RV dilation

15/
A primary reason for POCUS was to guide decision to perform paracentesis.
With these images, do you perform paracentesis immediately at the bedside (if you find a reasonable pocket)
A) Yes - diagnostic only
B) Yes - diagnostic and large volume
C) No
A primary reason for POCUS was to guide decision to perform paracentesis.
With these images, do you perform paracentesis immediately at the bedside (if you find a reasonable pocket)
A) Yes - diagnostic only
B) Yes - diagnostic and large volume
C) No
16/
(poll) What is the most likely contributor to the abdominal distension?
A) Ascites
B) GI obstruction
C) Intraabdominal mass
D) 2 or more of the above
(poll) What is the most likely contributor to the abdominal distension?
A) Ascites
B) GI obstruction
C) Intraabdominal mass
D) 2 or more of the above
17/
What would be your next step(s) in management at this point (open ended)
Case-wrap up to follow!
What would be your next step(s) in management at this point (open ended)
Case-wrap up to follow!
tagging POCUS friends/past participants:
@NephroP @DRsonosRD @laxswamy @DrGalenMD @cameron_baston @kyliebaker888 @RogerAlvarezDO @MikeRoseMDMPH @cianmcdermott @easypocus @bryanboling @virenkaul @pedrodammert @karthi8913 @trobertson8 @collinflan @TimRowesays @ArgaizR @Cometin007
@NephroP @DRsonosRD @laxswamy @DrGalenMD @cameron_baston @kyliebaker888 @RogerAlvarezDO @MikeRoseMDMPH @cianmcdermott @easypocus @bryanboling @virenkaul @pedrodammert @karthi8913 @trobertson8 @collinflan @TimRowesays @ArgaizR @Cometin007
What would be your next step(s) in management at this point? (open ended)
Case-wrap up to follow!
Case-wrap up to follow!
18/
POCUS findings
-Anechoic ascites
-Stomach: distended, fluid-filled. NG tube seen
-Small bowel: dilated, prominent valvuli conniventes, ineffective peristalsis
-Large bowel not seen
-Heterogeneous structure behind small bowel
-No comment on liver morphology
(KUB also shown)
POCUS findings
-Anechoic ascites
-Stomach: distended, fluid-filled. NG tube seen
-Small bowel: dilated, prominent valvuli conniventes, ineffective peristalsis
-Large bowel not seen
-Heterogeneous structure behind small bowel
-No comment on liver morphology
(KUB also shown)




19/
Integration: ascites was found, as expected on exam. No clear indication of cirrhosis. The findings were highly concerning for SBO. There may have been an abd mass seen, though not certain. Given the history, concerning for abd mass w malignant ascites and bowel obstruction.
Integration: ascites was found, as expected on exam. No clear indication of cirrhosis. The findings were highly concerning for SBO. There may have been an abd mass seen, though not certain. Given the history, concerning for abd mass w malignant ascites and bowel obstruction.
20/
NG placed for decompression
CT A/P: dilated stomach w retained contrast, dilated fluid-filled small bowel, no transition point. Low grade SBO vs ileus. Large mesenteric mass
Paracentesis performed (in peritoneum, not stomach): exudate, - cx, cytology + for malignant cells
NG placed for decompression
CT A/P: dilated stomach w retained contrast, dilated fluid-filled small bowel, no transition point. Low grade SBO vs ileus. Large mesenteric mass
Paracentesis performed (in peritoneum, not stomach): exudate, - cx, cytology + for malignant cells
21/
Diagnosis: mesenteric mass with malignant ascites and likely bowel obstruction.
Key Points
1) Gastric distension on POCUS
2) Sonographic findings of SBO
3) Role of POCUS in cases like this
Diagnosis: mesenteric mass with malignant ascites and likely bowel obstruction.
Key Points
1) Gastric distension on POCUS
2) Sonographic findings of SBO
3) Role of POCUS in cases like this
22/
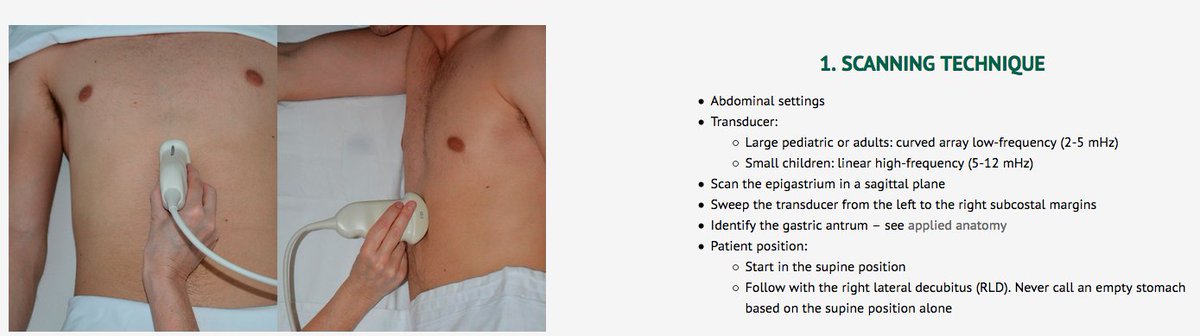
1) Gastric distension on POCUS
-For standardized technique gastricultrasound.org/Image%20Acquis…
-Normal volume depends on last meal - in fasting pt expected to be < 1.5 mL/kg
-R lat decubitus can move gas for better visualization
-distended stomach may prompt NG suction, further imaging
1) Gastric distension on POCUS
-For standardized technique gastricultrasound.org/Image%20Acquis…
-Normal volume depends on last meal - in fasting pt expected to be < 1.5 mL/kg
-R lat decubitus can move gas for better visualization
-distended stomach may prompt NG suction, further imaging
23/
Most of the literature on POCUS and gastric distension relates to implications of gastric distension in the anesthesia setting.
Limited evidence for sens/spec.
Suspect this finding is specific (present if seen clearly) but not sensitive (could be easily obscured by gas).
Most of the literature on POCUS and gastric distension relates to implications of gastric distension in the anesthesia setting.
Limited evidence for sens/spec.
Suspect this finding is specific (present if seen clearly) but not sensitive (could be easily obscured by gas).
24/
More resources on this
Great video lecture by @kyliebaker on GI POCUS @ThinkingCC
thinkingcriticalcare.com/2019/07/12/hr2…
And an article with a nice overview on common practical abd US applications in intensive care @Wilkinsonjonny @avkwong
healthmanagement.org/pdf/article-do…
More resources on this
Great video lecture by @kyliebaker on GI POCUS @ThinkingCC
thinkingcriticalcare.com/2019/07/12/hr2…
And an article with a nice overview on common practical abd US applications in intensive care @Wilkinsonjonny @avkwong
healthmanagement.org/pdf/article-do…
25/
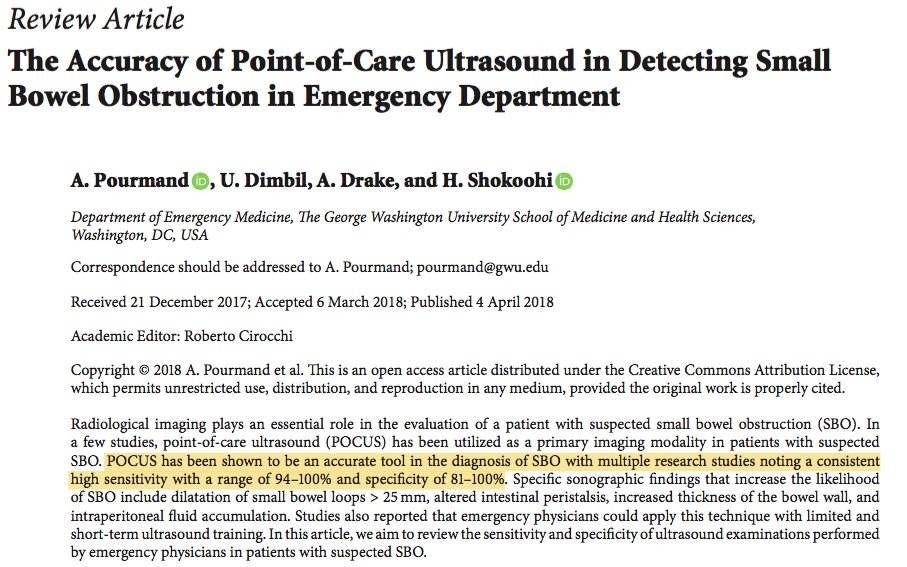
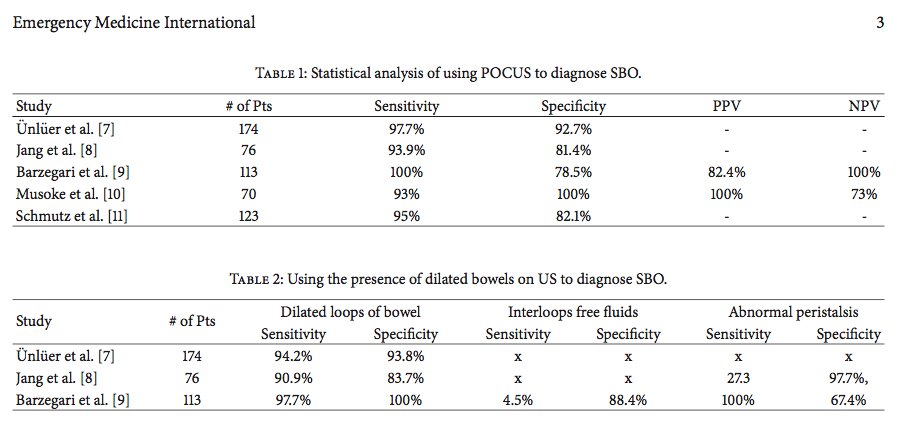
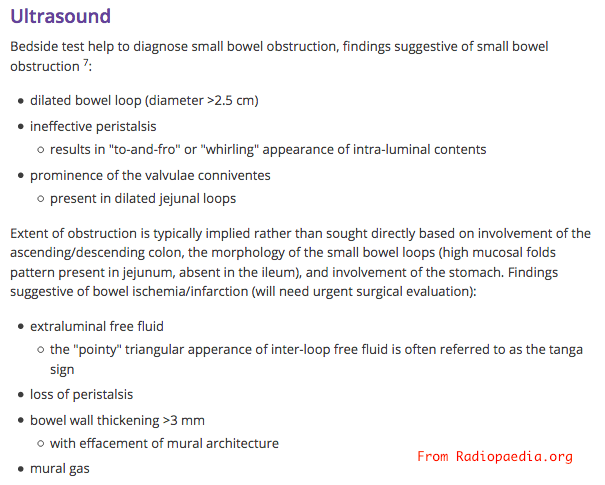
2) POCUS and SBO
-details on findings from radiopaedia.org/articles/small…
-review article here finds sensitivity 93-100% and specificity 78-100% of ED POCUS for SBO (with formal implementation programs). ncbi.nlm.nih.gov/pmc/articles/P…
2) POCUS and SBO
-details on findings from radiopaedia.org/articles/small…
-review article here finds sensitivity 93-100% and specificity 78-100% of ED POCUS for SBO (with formal implementation programs). ncbi.nlm.nih.gov/pmc/articles/P…
26/
3) Role of POCUS
With or w/o POCUS, the dx may be reached, but POCUS may expedite dx. As such, it is useful in the assessment of patients with abdominal distension when done with consideration of pre-test probabilities and possible findings.
(pre-POCUS polls shown here)
3) Role of POCUS
With or w/o POCUS, the dx may be reached, but POCUS may expedite dx. As such, it is useful in the assessment of patients with abdominal distension when done with consideration of pre-test probabilities and possible findings.
(pre-POCUS polls shown here)



27/
Thanks to all who participated @salmannaeem217 @jminardi21 @jtanguay11 @POCUS_Society @pedrodammert @cianmcdermott @iceman_ex @ArgaizR @Wilkinsonjonny @doctorthierry @PacoDaFi @Elennaro @NephroP @ThinkingCC @VirtueOfNothing
As always, we welcome any additional input!
Thanks to all who participated @salmannaeem217 @jminardi21 @jtanguay11 @POCUS_Society @pedrodammert @cianmcdermott @iceman_ex @ArgaizR @Wilkinsonjonny @doctorthierry @PacoDaFi @Elennaro @NephroP @ThinkingCC @VirtueOfNothing
As always, we welcome any additional input!