,
28 tweets,
19 min read
Read on Twitter
IVC image acquisition #IMPOCUS #MedTweetorial.
These 2 IVC M-mode images were obtained from the same patient 10 seconds apart. How could they be so different?
1/
These 2 IVC M-mode images were obtained from the same patient 10 seconds apart. How could they be so different?
1/
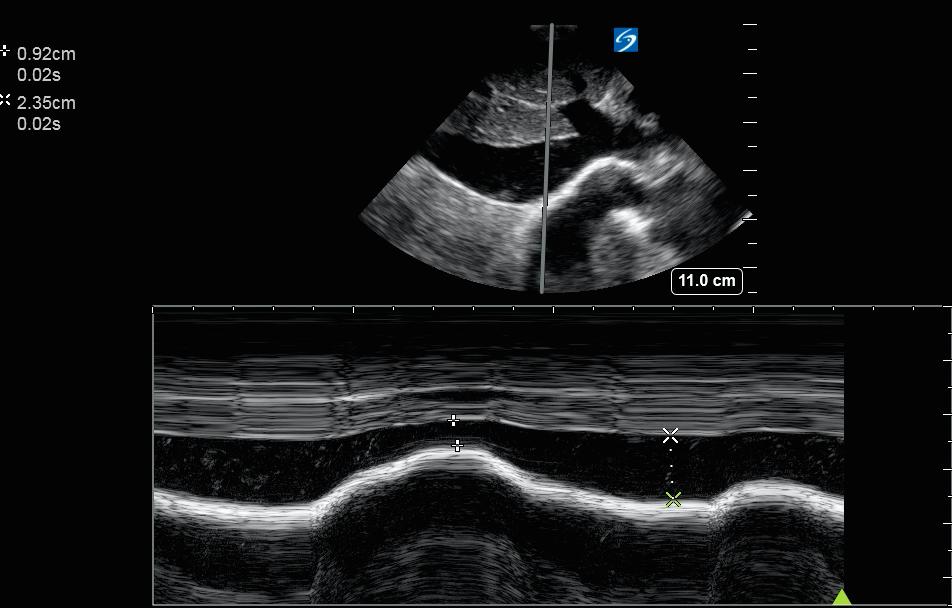
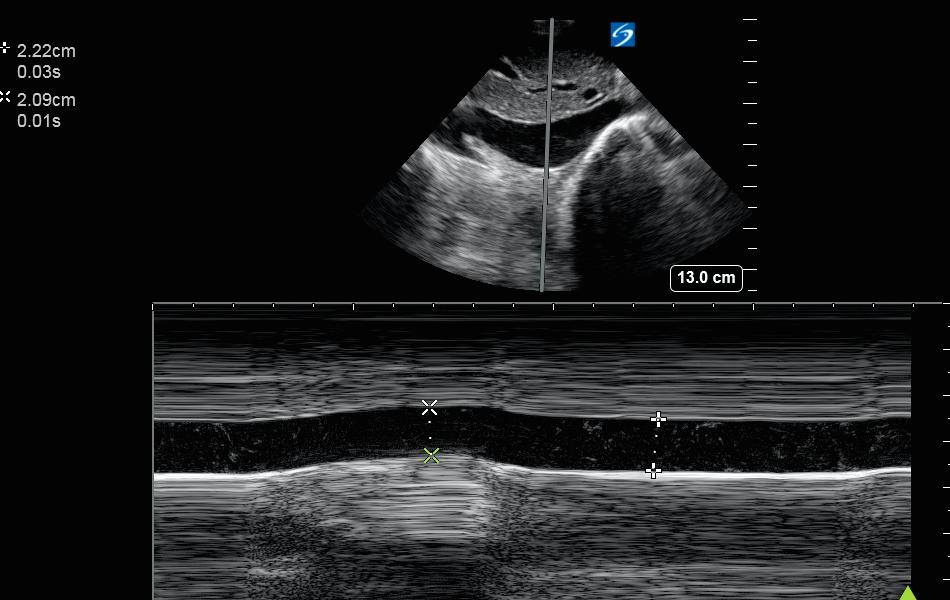
60 m with hx of COPD, HFpEF, admitted w LLL PNA s/p abx and 1 L LR. HR 118 BP 110/70. IVC US was performed as a piece of info in determining whether to administer more IVF.
Measurement 1: 2.35-->0.92 (65% collapse)
Measurement 2: 2.22-->2.09 (5% collapse)
Why so different?
2/
Measurement 1: 2.35-->0.92 (65% collapse)
Measurement 2: 2.22-->2.09 (5% collapse)
Why so different?
2/
First of all, how do you look at the IVC?
A common method is subxyphoid long axis, B mode or M mode. See below
-photo from emedicine.medscape.com/article/104401…
-excerpt from WikiM (wikem.org/wiki/IVC_ultra…) for a nice description
-an annotated sample B mode image and M mode image
3/
A common method is subxyphoid long axis, B mode or M mode. See below
-photo from emedicine.medscape.com/article/104401…
-excerpt from WikiM (wikem.org/wiki/IVC_ultra…) for a nice description
-an annotated sample B mode image and M mode image
3/

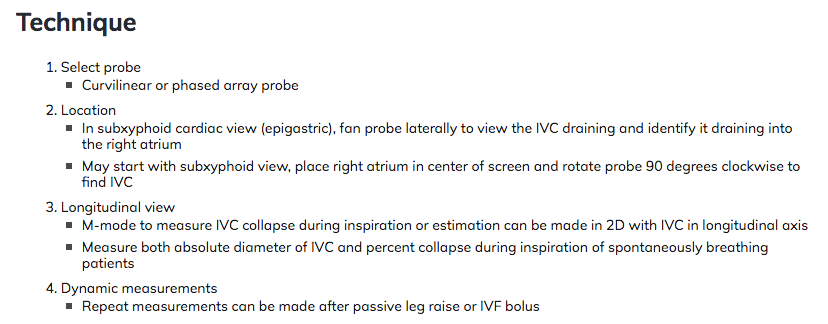
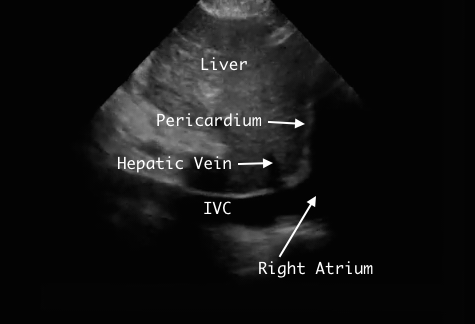
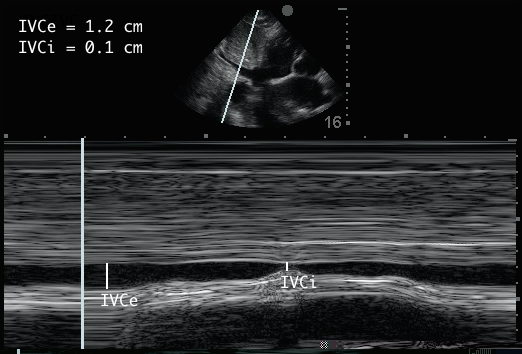
Max diameter (expiratory) and min diameter (inspiratory) can be measured, and % collapse can be calculated. A table can be used to estimate CVP (note we are talking spontaneously breathing pts)
Sounds easy, right?
Below we discuss a few of the many nuances involved in this.
4/
Sounds easy, right?
Below we discuss a few of the many nuances involved in this.
4/

Let's look at what exactly can lead to variation in images
1) Craniocaudal insp movement
2) Mediolateral insp movement
3) Nonuniform insp collapse
4) Variability in location of measurement (M mode)
5) Variation in breathing pattern
Which of the above are present in our pt?
5/
1) Craniocaudal insp movement
2) Mediolateral insp movement
3) Nonuniform insp collapse
4) Variability in location of measurement (M mode)
5) Variation in breathing pattern
Which of the above are present in our pt?
5/
Looking at M mode images above, some variability in location of measurement is seen (M mode cursor more caudal in second image) But otherwise is difficult to know with M-mode alone. So let’s look at the same view (subxyphoid, long axis) in B-mode
6/
6/
And with M mode cursor, for a reference
We see cranio-caudal insp movement, which narrows IVC in line with M-mode cursor, w/o narrowing the IVC itself much. We also see non-uniform collapse, greater at level of hepatic vein. These, in combo with different cursor placement, helps explain 2 different M-mode images
7/
7/
But what about other factors? Let's look at a transverse cut
8/
8/
And with B mode for reference
9/
9/
In these clips, we see
-non-uniform collapse (from the left posterior)
-medio-lateral movement (slight)
-cranio-caudal movement (evidenced by sliding of the hepatic vein cross section toward the IVC)
These can also contribute to variation between measurements.
10/
-non-uniform collapse (from the left posterior)
-medio-lateral movement (slight)
-cranio-caudal movement (evidenced by sliding of the hepatic vein cross section toward the IVC)
These can also contribute to variation between measurements.
10/
Variations in respiratory pattern can also change the results (ex: sniff vs. labored breathing vs quiet breathing). Literature and practice patterns are not entirely clear on a "best" approach to this. Overall, worth noting that more resp effort--> more inspiratory collapse.
11/
11/
So in this case, the following factors contributed to variation in the IVC M mode image
-Craniocaudal insp movement
-Mediolateral insp movement
-Nonuniform insp collapse
-Variability in location of measurement
12/
-Craniocaudal insp movement
-Mediolateral insp movement
-Nonuniform insp collapse
-Variability in location of measurement
12/
What approach(es) can we take to minimize variation
-Watch for craniocaudal movement in long axis
-Watch for mediolateral movement in transverse axis
-Many advise not using M-mode at all. If using M-mode, place cursor 2-3 cm below RA or 1 cm below hepatic vein
13/
-Watch for craniocaudal movement in long axis
-Watch for mediolateral movement in transverse axis
-Many advise not using M-mode at all. If using M-mode, place cursor 2-3 cm below RA or 1 cm below hepatic vein
13/
If you view the IVC in multiple views and consistent findings are present, the findings carry more weight.
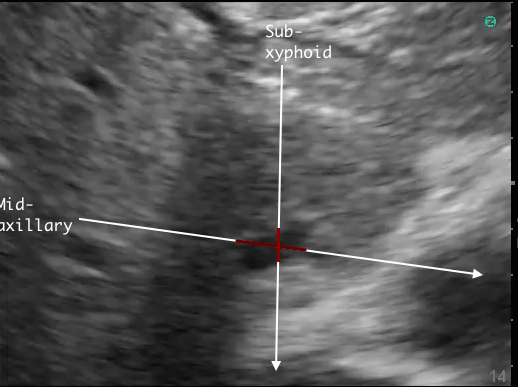
Where can you view the IVC? options include:
1) Subxyphoid, Long axis
2) Subxyphoid, Transverse axis
3) Midaxillary Line (“rescue view”), long or transverse
18/
Where can you view the IVC? options include:
1) Subxyphoid, Long axis
2) Subxyphoid, Transverse axis
3) Midaxillary Line (“rescue view”), long or transverse
18/
Keep in mind that collapsibility index may be an underestimate in midaxillary view, especially when IVC is more flat, due to overestimation of minimum diameter due to the plane in which the IVC is viewed (see image). These was assessed in this article journal.chestnet.org/article/S0012-…
19/
19/
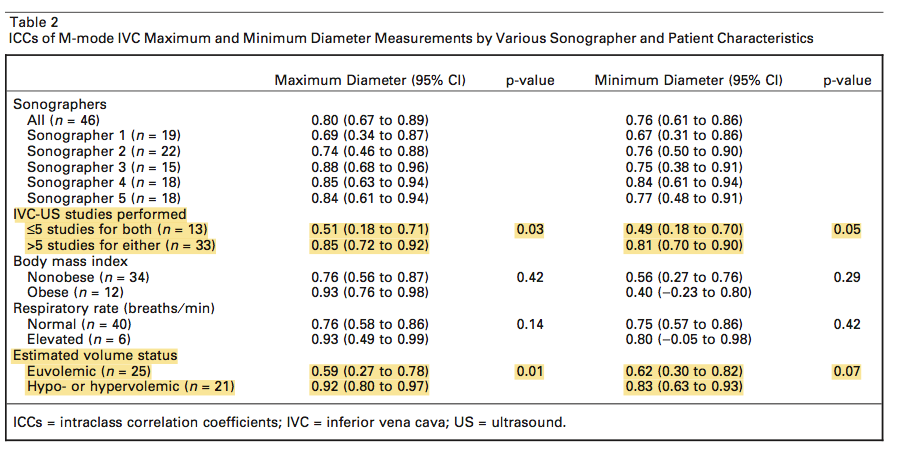
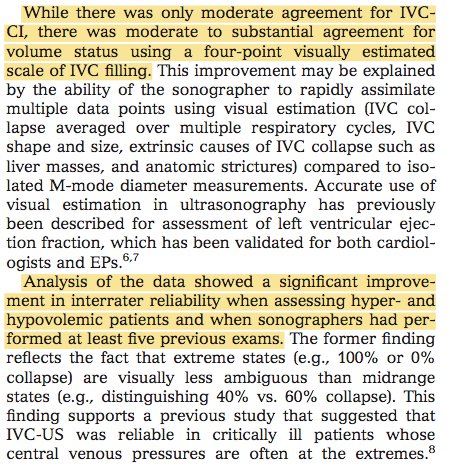
So how is inter-rater reliability for IVC- (US?
This study found reliability was higher at extremes of volume status, more operator experience (>5 IVC scans), and when a four-point visually estimated scale was used.
ncbi.nlm.nih.gov/pubmed/21414063 (openaccess)
20/
This study found reliability was higher at extremes of volume status, more operator experience (>5 IVC scans), and when a four-point visually estimated scale was used.
ncbi.nlm.nih.gov/pubmed/21414063 (openaccess)
20/
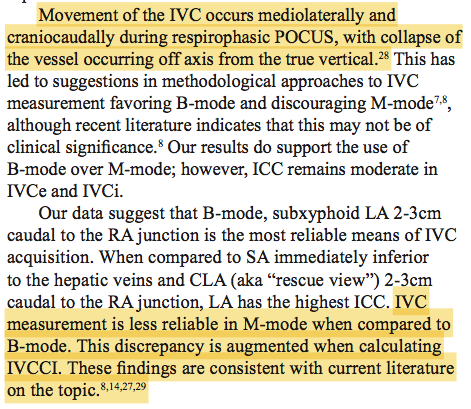
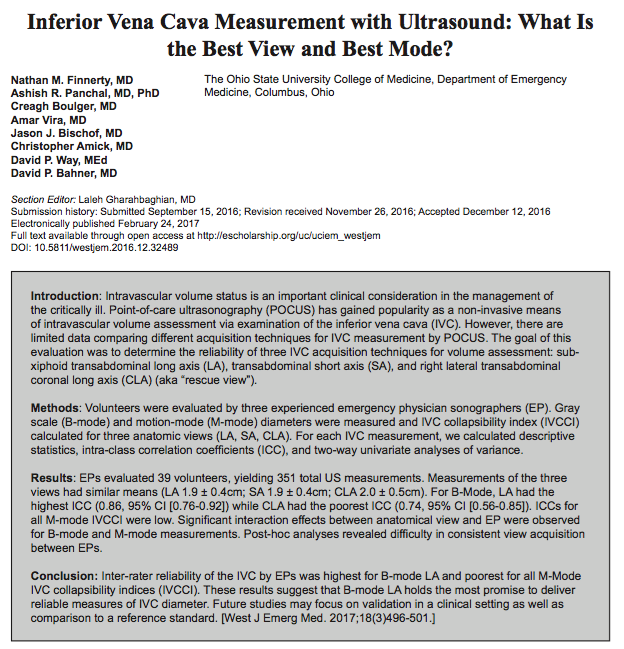
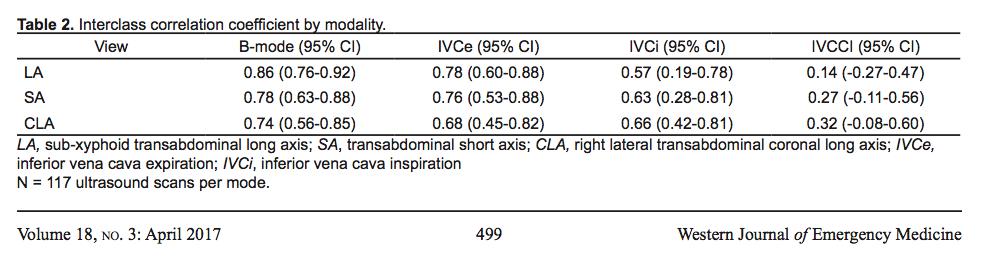
another study compared different methods/views, and found best reliability for the subxyphoid long axis view, and better reliability for B mode compared to M mode ncbi.nlm.nih.gov/pmc/articles/P… (open access). Variation was greatest when assessing IVC collapsibility index.
21/
21/
Putting it together for our case...
One M mode view reveals IVCe>2cm and IVCCI>50%. The other reveals IVCe>2c and minimal collapse. This would reflect intermediate to high CVP. However, data is inconsistent, and multiple causes for variation are noted.
22/
One M mode view reveals IVCe>2cm and IVCCI>50%. The other reveals IVCe>2c and minimal collapse. This would reflect intermediate to high CVP. However, data is inconsistent, and multiple causes for variation are noted.
22/
Best course of action would be to call this indeterminate, and not use it to sway decision-making substantially. IVC US can be extremely useful, especially in extremes, but it's important to recognize when not to put too much weight on POCUS findings, such as in this case.
23/
23/
Take home points
-IVC US is not easy.
-most useful in extremes.
-don't rely on 1 M-mode image. check B mode in subxyph long and short axis too.
-watch for craniocaudal + mediolateral movement.
-midaxillary view underestimates IVCCI.
-interpret findings in clinical context.
24/
-IVC US is not easy.
-most useful in extremes.
-don't rely on 1 M-mode image. check B mode in subxyph long and short axis too.
-watch for craniocaudal + mediolateral movement.
-midaxillary view underestimates IVCCI.
-interpret findings in clinical context.
24/

This is a complex discussion, even just focusing on acquisition. Integration of IVC US which would be an even lengthier discussion
We would love to hear opinions/viewpoints/experiences from #POCUS #IMPOCUS #MedTwitter community. We welcome disagreements and/or additions!
25/
We would love to hear opinions/viewpoints/experiences from #POCUS #IMPOCUS #MedTwitter community. We welcome disagreements and/or additions!
25/
Would love to hear opinions/viewpoints/experiences from #POCUS community @SonoInternist @DRsonosRD @G2Disrupt @IM_POCUS @buckeye_sanjay @kyliebaker888 @HeyDrNik @laxswamy @siddharth_dugar @Wilkinsonjonny @LMSaxhaug @iceman_ex @curromir @greggmccordMD @PeterMarogi @Cometin007
as always, we advise posting any replies to first tweet of thread to keep the thread organized and easy to follow.
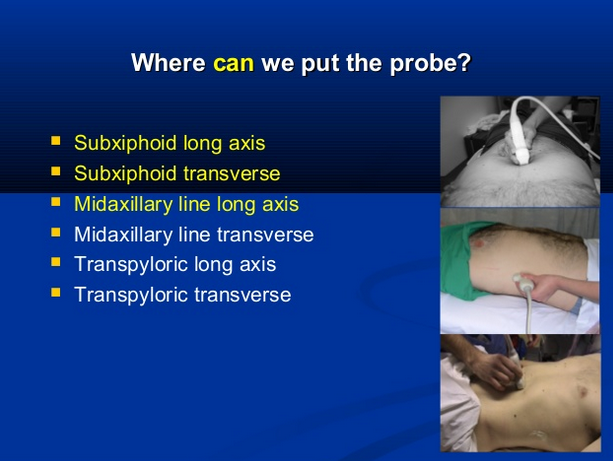
Adding in here a slide w some photos on placement of the probe at each of these sites
From a nice slide set: "IVC Ultrasound, the Ultimate Myth"
slideshare.net/oliflower/just…
(c/o @justinbowra, and thanks to @kyliebaker888 & her team for one of the probe placement photos)
From a nice slide set: "IVC Ultrasound, the Ultimate Myth"
slideshare.net/oliflower/just…
(c/o @justinbowra, and thanks to @kyliebaker888 & her team for one of the probe placement photos)
*should read with M-mode cursor for reference