1/
Treating metabolic acidosis, brief tweetorial #UncleBob
Today’s @CPSolvers Virtual Morning Report: complicated patient w/ an AKI. Labs: normal gap acidosis w/ inadequate compensation. Whether to treat the acidosis created some controversy
@tony_breu @kidney_boy
Treating metabolic acidosis, brief tweetorial #UncleBob
Today’s @CPSolvers Virtual Morning Report: complicated patient w/ an AKI. Labs: normal gap acidosis w/ inadequate compensation. Whether to treat the acidosis created some controversy
@tony_breu @kidney_boy
2/
Labs: Na 124/K 5.1//Cl 103/HCO3 9/BUN 80/creat 8.1
Known diarrhea with negative urine anion gap
ABG pH 7.02/ pCO2 29/ pO2 80/ Bicarb 8
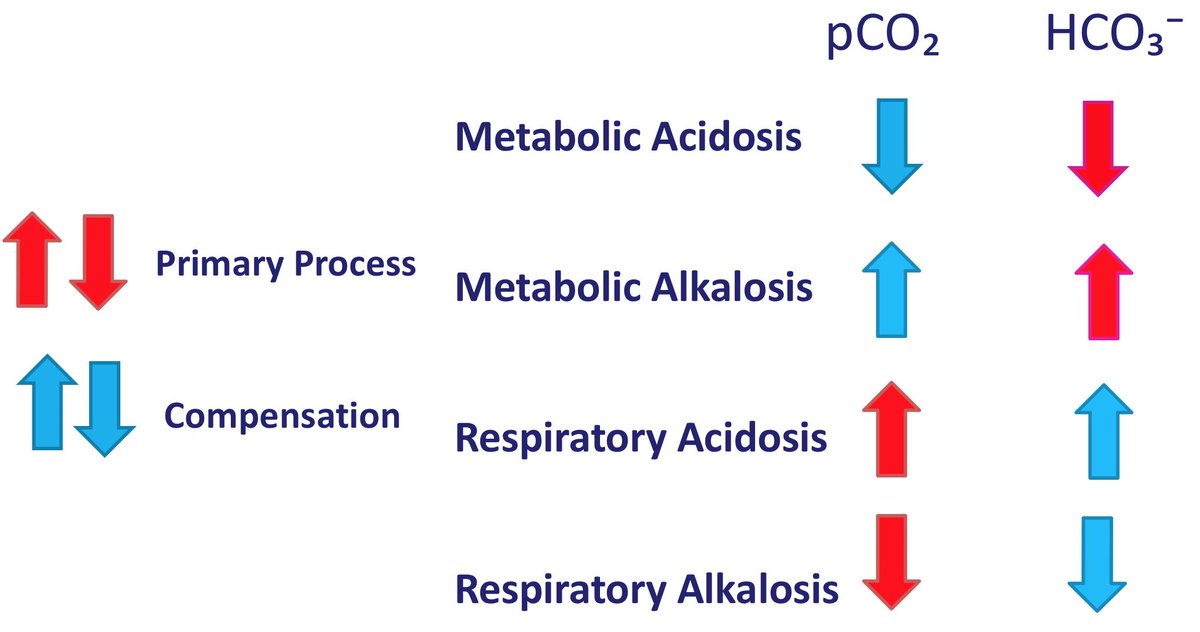
So the patient has a normal gap metabolic acidosis (severe) w/ resp acidosis - Winter's formula 8 times 1.5 = 12 + 8 +/- 2 = 18 - 22
Labs: Na 124/K 5.1//Cl 103/HCO3 9/BUN 80/creat 8.1
Known diarrhea with negative urine anion gap
ABG pH 7.02/ pCO2 29/ pO2 80/ Bicarb 8
So the patient has a normal gap metabolic acidosis (severe) w/ resp acidosis - Winter's formula 8 times 1.5 = 12 + 8 +/- 2 = 18 - 22
3/
First major teaching point, the original Winter's equation used only the ABG - so choose the ABG bicarb
Albert, M.S., DELL, R.B. and WINTERS, R.W., 1967. Quantitative displacement of acid-base equilibrium in metabolic acidosis. Annals of internal medicine, 66(2), pp.312-322.
First major teaching point, the original Winter's equation used only the ABG - so choose the ABG bicarb
Albert, M.S., DELL, R.B. and WINTERS, R.W., 1967. Quantitative displacement of acid-base equilibrium in metabolic acidosis. Annals of internal medicine, 66(2), pp.312-322.
4/
Second teaching point - should we give bicarbonate? A wonderful article in JASN addresses this issue nicely
Sabatini, S. and Kurtzman, N.A., 2009. Bicarbonate therapy in severe metabolic acidosis. Journal of the American Society of Nephrology, 20(4), pp.692-695.
Second teaching point - should we give bicarbonate? A wonderful article in JASN addresses this issue nicely
Sabatini, S. and Kurtzman, N.A., 2009. Bicarbonate therapy in severe metabolic acidosis. Journal of the American Society of Nephrology, 20(4), pp.692-695.
5/
My understanding: Always treat normal gap acidosis w/ a goal bicarb of 22. Rarely treat increased anion gap acidosis - virtually never for DKA, only w/ a dangerous pH in lactic acidosis. Experts disagree on the definition of dangerous pH. Apparently no convincing studies
My understanding: Always treat normal gap acidosis w/ a goal bicarb of 22. Rarely treat increased anion gap acidosis - virtually never for DKA, only w/ a dangerous pH in lactic acidosis. Experts disagree on the definition of dangerous pH. Apparently no convincing studies
6/
The way I give bicarbonate. Let's assume the patient was an 80 kg man. The bicarbonate space is the same as total body water or ~ 50%, therefore 40 liters. The deficit is 13 mEq per liter so 13*40=520 mEq.
The way I give bicarbonate. Let's assume the patient was an 80 kg man. The bicarbonate space is the same as total body water or ~ 50%, therefore 40 liters. The deficit is 13 mEq per liter so 13*40=520 mEq.
7/
In this pt I would add 3 amps of sodium bicarbonate to a liter of D5/W (assume no thiamine deficiency or phosphate deficiency). Since the patient had signs of volume depletion, I would run at 125 or 150 cc/ hour, but might even run the first liter in much faster.
In this pt I would add 3 amps of sodium bicarbonate to a liter of D5/W (assume no thiamine deficiency or phosphate deficiency). Since the patient had signs of volume depletion, I would run at 125 or 150 cc/ hour, but might even run the first liter in much faster.
8/
After around 3 liters, the bicarbonate should be close to target.
If diarrhea persists, then might need continued bicarbonate.
I hope this is helpful.
Remember the aggressive treatment of metabolic acidosis ONLY applies to NAGMA
After around 3 liters, the bicarbonate should be close to target.
If diarrhea persists, then might need continued bicarbonate.
I hope this is helpful.
Remember the aggressive treatment of metabolic acidosis ONLY applies to NAGMA