
#MedTwitter how often do you use 𝐏𝐫𝐨𝐜𝐚𝐥𝐜𝐢𝐭𝐨𝐧𝐢𝐧 ?
A thread on 𝐏𝐫𝐨𝐜𝐚𝐥𝐜𝐢𝐭𝐨𝐧𝐢𝐧 for those interested 😉
#MedEd #MedStudentTwitter #oncology #hematology #tweetorial
A thread on 𝐏𝐫𝐨𝐜𝐚𝐥𝐜𝐢𝐭𝐨𝐧𝐢𝐧 for those interested 😉
#MedEd #MedStudentTwitter #oncology #hematology #tweetorial
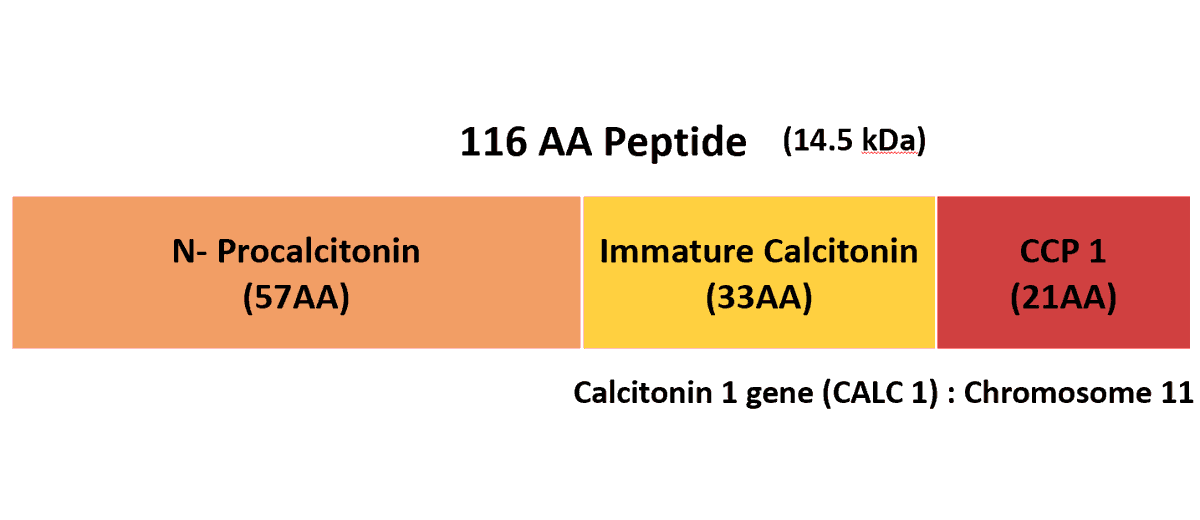
⚡️Procalcitonin as the name suggests is a precursor of the hormone calcitonin
⚡️Coded by the CALC 1 gene on Chr 11,its a 116AA peptide
⚡️PrePCT >> PCT >> Calcitonin
⚡️Bact inf=⬆️IL6⬆️TNFa⬆️IL1b=⬆️Productn of PCT
⚡️Coded by the CALC 1 gene on Chr 11,its a 116AA peptide
⚡️PrePCT >> PCT >> Calcitonin
⚡️Bact inf=⬆️IL6⬆️TNFa⬆️IL1b=⬆️Productn of PCT
⚡️Normal PCT in health <0.1ng/ml
⚡️In patients with bacterial infections PCT ⬆️ corelates with severity of infection
⚡️PCT starts to⬆️3-4hrs following an infection,
peaks at ~12 hrs post infection.
⚡️In patients with bacterial infections PCT ⬆️ corelates with severity of infection
⚡️PCT starts to⬆️3-4hrs following an infection,
peaks at ~12 hrs post infection.
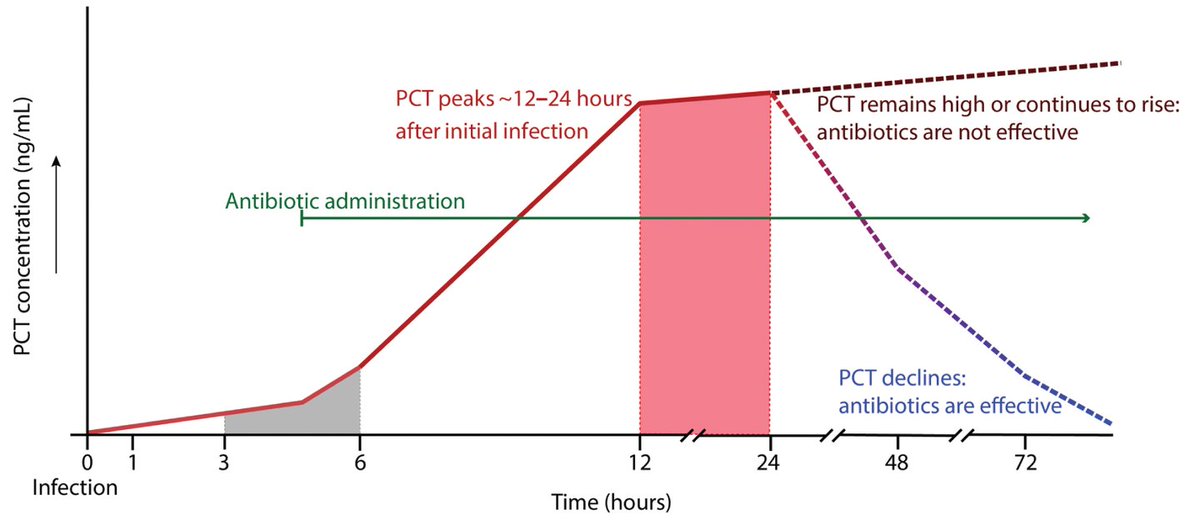
⚡️The image below beautifully summarizes the kinetic profile of biomarkers in bacterial infections
⚡️As seen CRP rises and peaks later and stays elevated for a longer time even after resolution of infection.
⚡️As seen CRP rises and peaks later and stays elevated for a longer time even after resolution of infection.

⚡️But there are other reasons for an ⬆️PCT like major surgery, burns, severe trauma etc.
Cardiogenic shock also l/t ⬆️PCT
⚡️That's where serial monitoring becomes important.
The levels wont stay elevated in these conditions.
⚡️Med Ca thyroid and SCLC l/t ⬆️PCT(dysreg productn)
Cardiogenic shock also l/t ⬆️PCT
⚡️That's where serial monitoring becomes important.
The levels wont stay elevated in these conditions.
⚡️Med Ca thyroid and SCLC l/t ⬆️PCT(dysreg productn)
⚡️Similarly a Normal PCT doesn't r/o bact infection. Localized infections like empyema, osteomyelitis can have normal PCT.
⚡️PCT is quantified by immunoassay technique. The 1st commercial kit was BRAHMS PCT LIA.
⚡️PCT Kryptor an automated assay was FDA approved in 2008
⚡️PCT is quantified by immunoassay technique. The 1st commercial kit was BRAHMS PCT LIA.
⚡️PCT Kryptor an automated assay was FDA approved in 2008
⚡️Semiquantitative strip tests use immunochromatography and serve as point of care tests for PCT.

⚡️PCT guided antibiotic therapy was evaluated in the PRORATA trial and it was effective in⬇️antibiotic exposure.
⚡️However, ⬆️PCT is not a good marker for intensifying antibiotics (PASS study data)
⚡️However, ⬆️PCT is not a good marker for intensifying antibiotics (PASS study data)

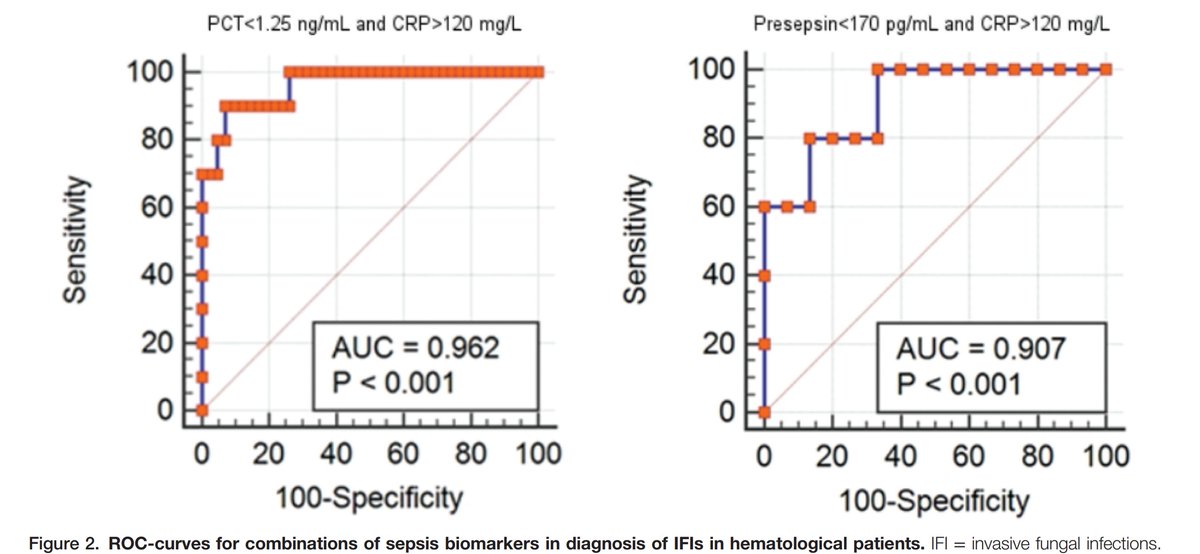
⚡️A combination of CRP and PCT may prove helpful in distinguishing bacterial vs IFI in patients with febrile neutropenia.
⬇️PCT and ⬆️CRP should lead to a high suspicion of IFI in patients with neutropenia.
⬇️PCT and ⬆️CRP should lead to a high suspicion of IFI in patients with neutropenia.
References :
dx.doi.org/10.1097/HS9.00…
Meisner M. Procalcitonin -Biochemistry and Clinical
Diagnosis. ISBN
PRORATA trial ; Lancet 2010
dx.doi.org/10.1097/HS9.00…
Meisner M. Procalcitonin -Biochemistry and Clinical
Diagnosis. ISBN
PRORATA trial ; Lancet 2010
@SujayRainchwar @sujeethemat @IJMPOofficial @SChellapuram @NutanJoshi27 @rahulbhargavadr @MayoClinicINFD @satya_yadav @IDSAInfo @ID_fellows @MedTweetorials @MedTweetsHQ @docsamdeshmukh @BollamRajesh4 @PHOJournal
• • •
Missing some Tweet in this thread? You can try to
force a refresh


