Let's talk about something common, hard to treat, and often misunderstood: CHRONIC BLOATING AND DISTENSION!
A 🧵 summarizing from the excellent @AGA_CGH article cghjournal.org/article/S1542-…
#GI #GITwitter #motility #IBS #DGBI #FGID #microbiome #health #MedEd
A 🧵 summarizing from the excellent @AGA_CGH article cghjournal.org/article/S1542-…
#GI #GITwitter #motility #IBS #DGBI #FGID #microbiome #health #MedEd
🟢Bloating: subjective sensation of gassiness, trapped💨, or a feeling of pressure or being distended w/o obvious visible distension.
🟢Distension: objective physical manifestation of an⬆️in abdominal girth. Patients commonly say they look like 🎈 or 🤰
🟢Distension: objective physical manifestation of an⬆️in abdominal girth. Patients commonly say they look like 🎈 or 🤰
Bloating and distension are COMMON
🔴16-31% in the general population
🔴Women > men
🔴66-99% in #IBS
🔴IBS-C > IBS-D
🟢Bloating and distension are distressing to patients and ⬇️quality of life
🔴16-31% in the general population
🔴Women > men
🔴66-99% in #IBS
🔴IBS-C > IBS-D
🟢Bloating and distension are distressing to patients and ⬇️quality of life
Many patients believe their bloating/distension is caused by⬆️gas but this is very rarely true! 💨
CT scans show gas ⬆️ in only 25% of patients with #DGBI during an episode of abdominal distension or following consumption of a “high-flatulence” diet.
⬇️Normal #gas production
CT scans show gas ⬆️ in only 25% of patients with #DGBI during an episode of abdominal distension or following consumption of a “high-flatulence” diet.
⬇️Normal #gas production

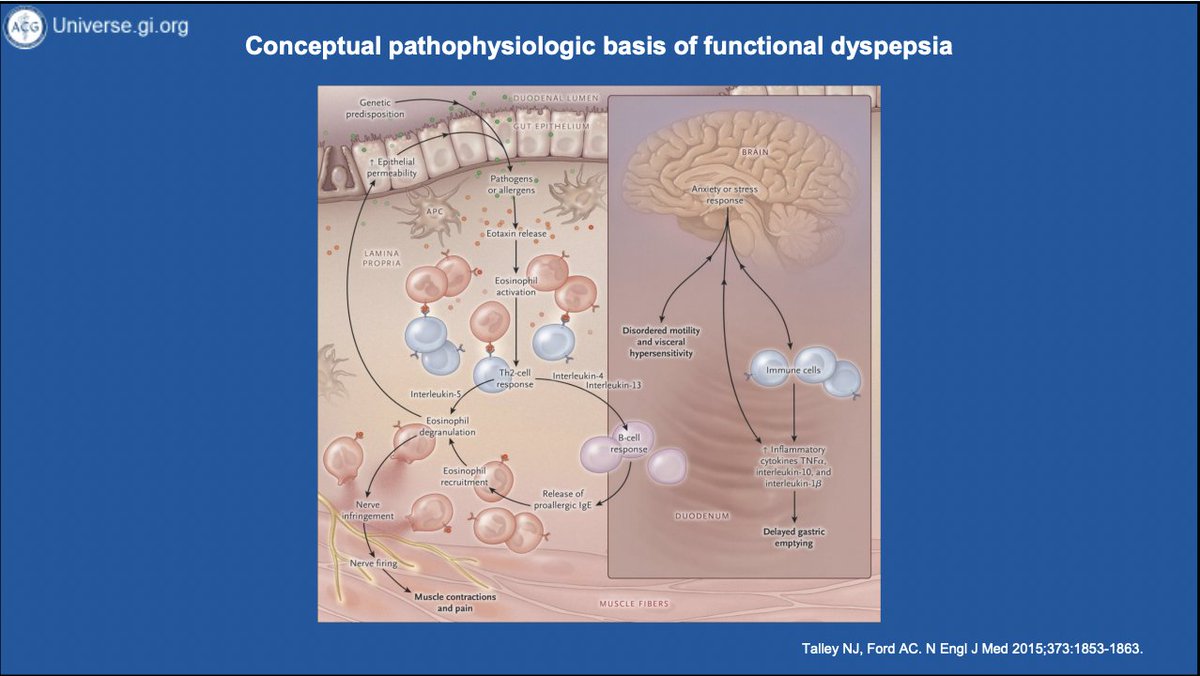
So what causes pathologic bloating/distension? Lots of things! And it's not always due to #GI dysfunction! Here's a nice list⬇️⬇️⬇️


Important factors
🟠#SIBO + carbohydrate (eg lactose, fructose) malabsorption
🟠Altered #gut #microbiome (❓⬇️Ruminococcaceae and Eubacteriaceae)
🟠dysmotility (gastroparesis, CIPO, scleroderma)
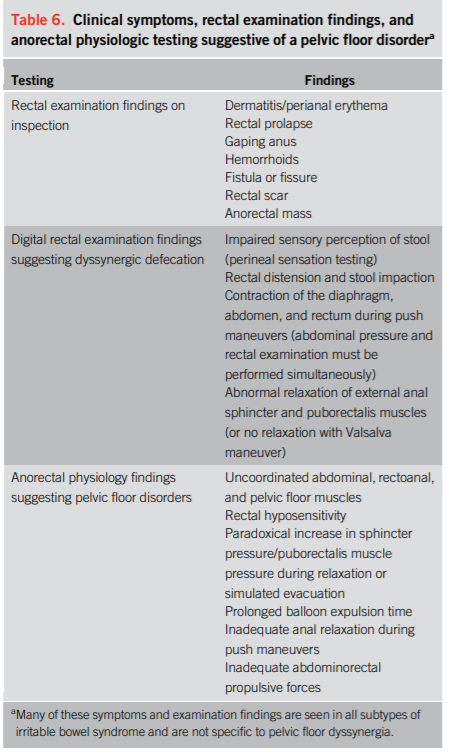
🟠pelvic floor dysfunction
🟠visceral hypersensitivity
🟠abdominophrenic dyssynergia
🟠#SIBO + carbohydrate (eg lactose, fructose) malabsorption
🟠Altered #gut #microbiome (❓⬇️Ruminococcaceae and Eubacteriaceae)
🟠dysmotility (gastroparesis, CIPO, scleroderma)
🟠pelvic floor dysfunction
🟠visceral hypersensitivity
🟠abdominophrenic dyssynergia
Abdominophrenic dyssynergia is *very common* in patients w bloating/distension, especially in functional bloating!
Normal:💨 ▶️diaphragm relaxes, and the anterior abdominal muscles contract
AD:💨 ▶️diaphragm contracts, and the anterior abdominal wall muscles relax
Normal:💨 ▶️diaphragm relaxes, and the anterior abdominal muscles contract
AD:💨 ▶️diaphragm contracts, and the anterior abdominal wall muscles relax

Don't forget the diagnosis of functional abdominal bloating and distension! This is common and underdiagnosed!
Biofeedback can be very helpful!
Biofeedback can be very helpful!

How should we work up chronic bloating and distension? Here's a start! ⬇️⬇️⬇️

Treatments
Diet
🟢artificial sweeteners⬆️💨
🟢FODMAPs (fermentable oligo-, di-, and monosaccharides) are common culprits
Probiotics
🟢L. sporogens/Bacillus coagulans had and Bifidobacterium species have been shown to improve bloating in #IBS
Diet
🟢artificial sweeteners⬆️💨
🟢FODMAPs (fermentable oligo-, di-, and monosaccharides) are common culprits
Probiotics
🟢L. sporogens/Bacillus coagulans had and Bifidobacterium species have been shown to improve bloating in #IBS

Meds
🟢Rifaximin treats bloating in #IBS and #SIBO
🟢Antispasmodics (if sx are from💨)
🟢Secretagogues (lubiprostone, linaclotide, plecanatide) in #IBS-C
🟢Prokinetics: not much data, but🤔neostigmine, pyridostigmine, prucalopride, and tegaserod
🟢Rifaximin treats bloating in #IBS and #SIBO
🟢Antispasmodics (if sx are from💨)
🟢Secretagogues (lubiprostone, linaclotide, plecanatide) in #IBS-C
🟢Prokinetics: not much data, but🤔neostigmine, pyridostigmine, prucalopride, and tegaserod
Meds
🟢Neuromodulators/antidepressants: amitryptiline, escitalopram, and buspirone in #FD; citalopram in #IBS
Other
🟢Biofeedback
🟢Pelvic floor physical therapy
🟢Peppermint oil
🟢Rikkunshito
🟢Hypnosis
🟢Neuromodulators/antidepressants: amitryptiline, escitalopram, and buspirone in #FD; citalopram in #IBS
Other
🟢Biofeedback
🟢Pelvic floor physical therapy
🟢Peppermint oil
🟢Rikkunshito
🟢Hypnosis
That's all folks! Some takeaways!
🎈bloating is COMMON
🎈MANY different causes
🎈Don't forget non-GI etiologies
🎈Pursue appropriate workup
🎈GIVE PTS A DIAGNOSIS! Don't forget functional B/D!
🎈Lots of treatment options including diet,💊, peppermint oil, and behavioral therapy
🎈bloating is COMMON
🎈MANY different causes
🎈Don't forget non-GI etiologies
🎈Pursue appropriate workup
🎈GIVE PTS A DIAGNOSIS! Don't forget functional B/D!
🎈Lots of treatment options including diet,💊, peppermint oil, and behavioral therapy
• • •
Missing some Tweet in this thread? You can try to
force a refresh