A little late but better late than never! ⌚️ Here's a recap of @AmCollegeGastro Virtual Grand Rounds by @ScottGabbardMD on...... FUNCTIONAL DYSPEPSIA!
🤢🤢🤢
This is a VERY common entity that is underdiagnosed! #MedTwitter take notice!
#GITwitter #GI #gut
🤢🤢🤢
This is a VERY common entity that is underdiagnosed! #MedTwitter take notice!
#GITwitter #GI #gut

DYSPEPSIA = epigastric #pain. (can be associated with any other upper #GI symptom such as epigastric fullness, nausea, vomiting, or heartburn).
Dyspepsia is COMMON, and most cases are FUNCTIONAL (i.e., caused by brain-gut axis dysfunction)!
Dyspepsia is COMMON, and most cases are FUNCTIONAL (i.e., caused by brain-gut axis dysfunction)!


Like all disorders of gut-brain interactions FD pathophysiology is❌completely understood, but is thought to be complex+multifactorial. Components include
🤢disrupted duodenal barrier
🤢altered duodenal #microbiome
🤢dysmotility
🤢visceral hypersensitivity
🤢psychosocial stress
🤢disrupted duodenal barrier
🤢altered duodenal #microbiome
🤢dysmotility
🤢visceral hypersensitivity
🤢psychosocial stress
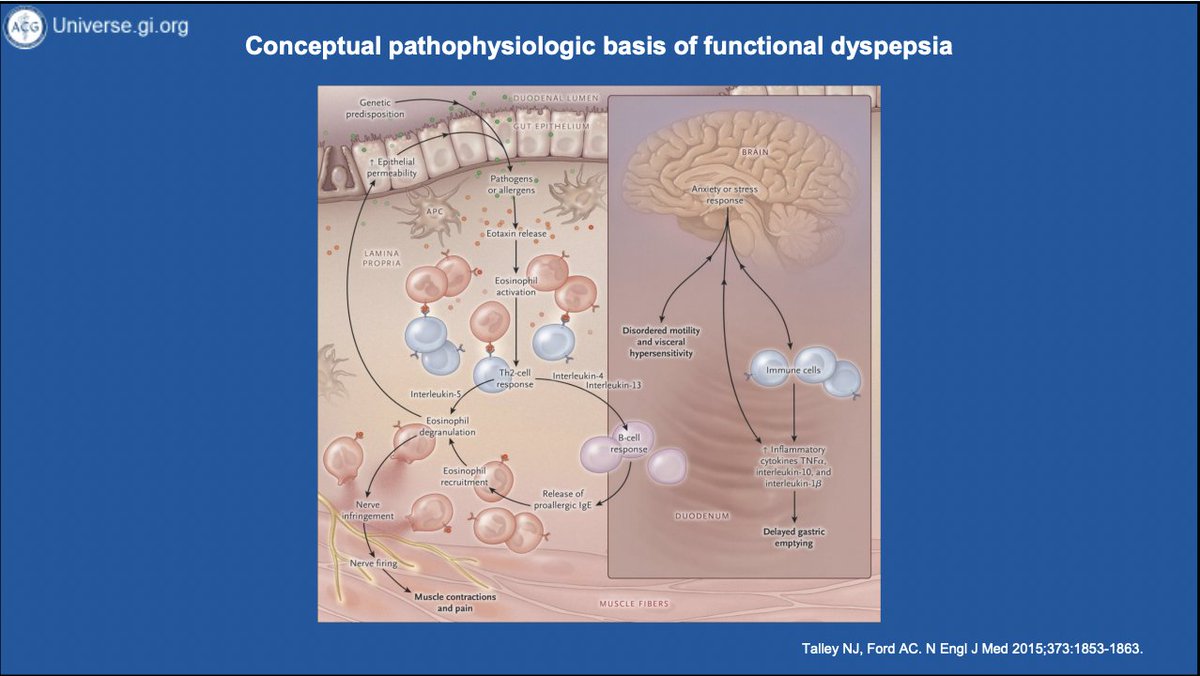
There is poor correlation btwn delayed gastric emptying+FD symptoms. In fact rapid emptying is MORE common than delayed in FD.We still don't completely understand the link btwn emptying+sx but FD and gastroparesis likely exist on a spectrum of gastroduodenal neuromuscular dysfxn



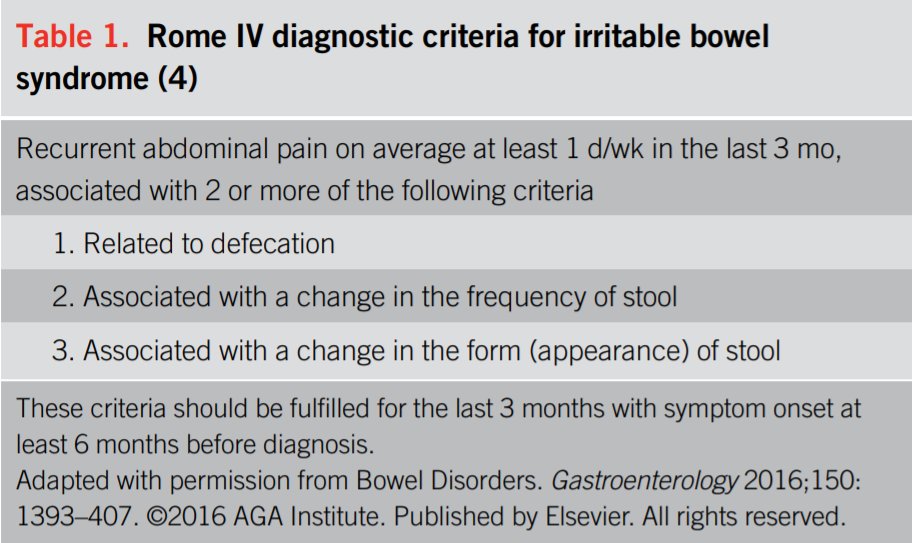
Diagnosis of functional dyspepsia can be made with the @RomeFoundation criteria. It is NOT a diagnosis of exclusion.
Two subtypes:
🤢Postprandial distress syndrome
🔥Epigastric pain syndrome
Two subtypes:
🤢Postprandial distress syndrome
🔥Epigastric pain syndrome



NOT all patients with dyspepsia need endoscopy. Here are some helpful tips to help decide which patients should get scoped⬇️⬇️⬇️


Test all patients with dyspepsia for H. pylori and treat accordingly!


Before treating functional dyspepsia, we must EDUCATE patients on the diagnosis!
🤢Tell them they have FD!
🤢No it's not #IBS! (Though many have both!)
🤢Describe as a "nerve disorder of the stomach" and discuss brain-gut axis 🧠
🤢Tell them they have FD!
🤢No it's not #IBS! (Though many have both!)
🤢Describe as a "nerve disorder of the stomach" and discuss brain-gut axis 🧠



🤢If FD is anything like #IBS, it may get better and even completely resolve over time
🤢FD does NOT ⬇️survival
🤢We have LOTS of treatment options including neuromodulators and behavioral therapies!
🤢FD does NOT ⬇️survival
🤢We have LOTS of treatment options including neuromodulators and behavioral therapies!



Once again, test for and treat H. pylori in patients with dyspepsia! If they have ongoing symptoms (after confirming eradication), it's probably FD! 🦠

Comparison of treatment for functional dyspepsia.
(Note, the antipsychotics sulpiride and levosulpiride with data for FD are not available in the US)
(Note, the antipsychotics sulpiride and levosulpiride with data for FD are not available in the US)

Neuromodulators: acting on 🧠 and gut!
💊TCAs
💊Buspirone
💊 Mirtazapine
💊TCAs
💊Buspirone
💊 Mirtazapine



Prokinetics may work in select patients.

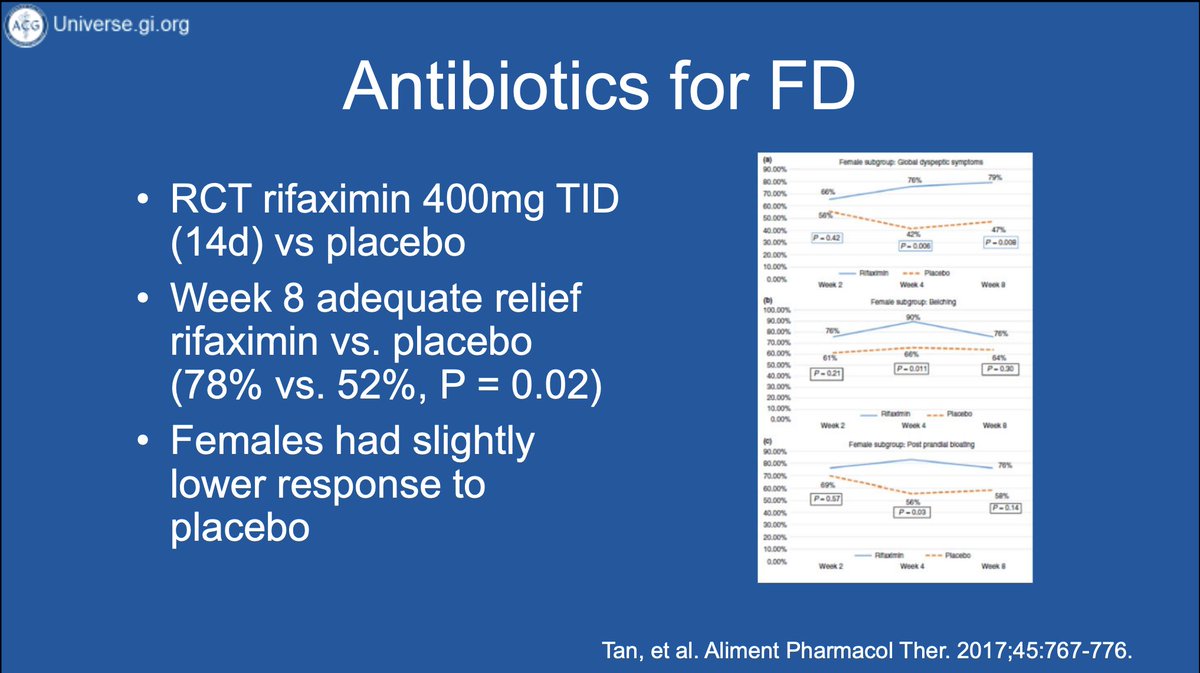
Antibiotics? Rifaximin is superior to placebo in resolving symptoms.
Supplements
💊STW5
💊Peppermint oil (want duodenal release so doesn't exacerbate GERD!)
💊capsaicin 🌶️🌶️🌶️
💊STW5
💊Peppermint oil (want duodenal release so doesn't exacerbate GERD!)
💊capsaicin 🌶️🌶️🌶️



Other therapies
✅acupuncture
✅behavioral therapy (including #hypnosis): NNT = 3⃣so we should be offering to everyone!!!
✅acupuncture
✅behavioral therapy (including #hypnosis): NNT = 3⃣so we should be offering to everyone!!!



What do the experts do? Here's @ScottGabbardMD's approach⬇️⬇️⬇️
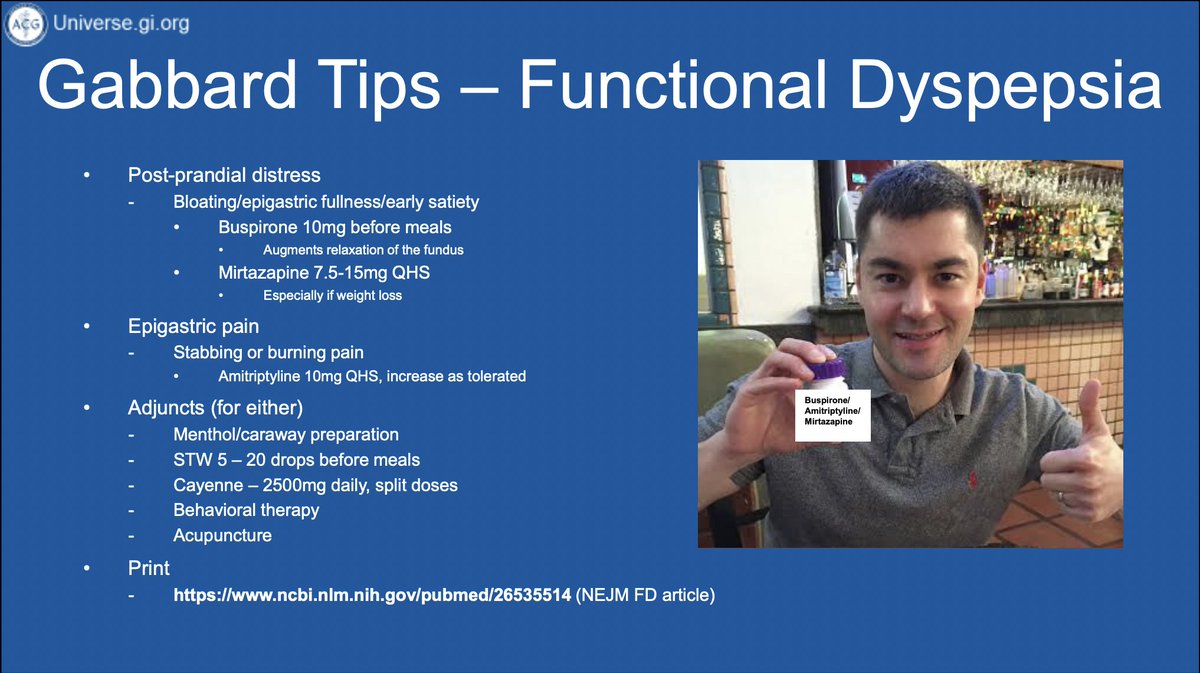
What have I done in my primary care clinic?
🧠given POSITIVE dx from @RomeFoundation criteria
🧠EDUCATED on brain-gut axis
🧠encouraged BEHAVIORAL therapy
🧠treated anxiety/depression preferentially w buspirone, mirtazapine, SNRIs, or TCAs depending on pain!
🧠peppermint oil!
🧠given POSITIVE dx from @RomeFoundation criteria
🧠EDUCATED on brain-gut axis
🧠encouraged BEHAVIORAL therapy
🧠treated anxiety/depression preferentially w buspirone, mirtazapine, SNRIs, or TCAs depending on pain!
🧠peppermint oil!
Thanks to @AmCollegeGastro, @ScottGabbardMD, and @AfrinKamalMD for the 🔥 #GIHomeschooling learning!
#GITwitter #GI #gut #motility #microbiome
#GITwitter #GI #gut #motility #microbiome
And a timely encore!
https://twitter.com/yuyingmd/status/1368611287815643141
@JCPetrov per our convo today!
• • •
Missing some Tweet in this thread? You can try to
force a refresh