This thread is directed to all of you searching for plasma donors and/or amplifying requests for plasma donation, but most importantly, for physicians suggesting plasma donation, or patients’ families demanding #ConvalescentPlasma treatment for their loved ones.
Over the past year and more, we have had #ConvalescentPlasma dominating conversations about #COVID_19 treatment. Families have run from pillar to post trying to find a compatible donor. We’ve had celebrities urging people to donate.
Importantly, we’ve had heartbroken families feel guilty about not having been able to identify a suitable donor in time to save their loved one’s life. This thread is meant for all of them.
Why did people think #ConvalescentPlasma will help? It is based on the theory that patients who get infected with #SARSCov2 develop antibodies to the infection, which will protect them for some time from getting reinfected.
And that these antibodies, if transfused to someone who has active #COVID_19 will fight the infection using these antibodies. Theoretically, it makes a lot of sense.
But that’s not how we evaluate new treatments. For any new treatment to be proven to be better than the existing standard of care, we need to show in a randomized controlled trial (RCT) that it is indeed superior. This is the gold standard for any new intervention to be evaluated
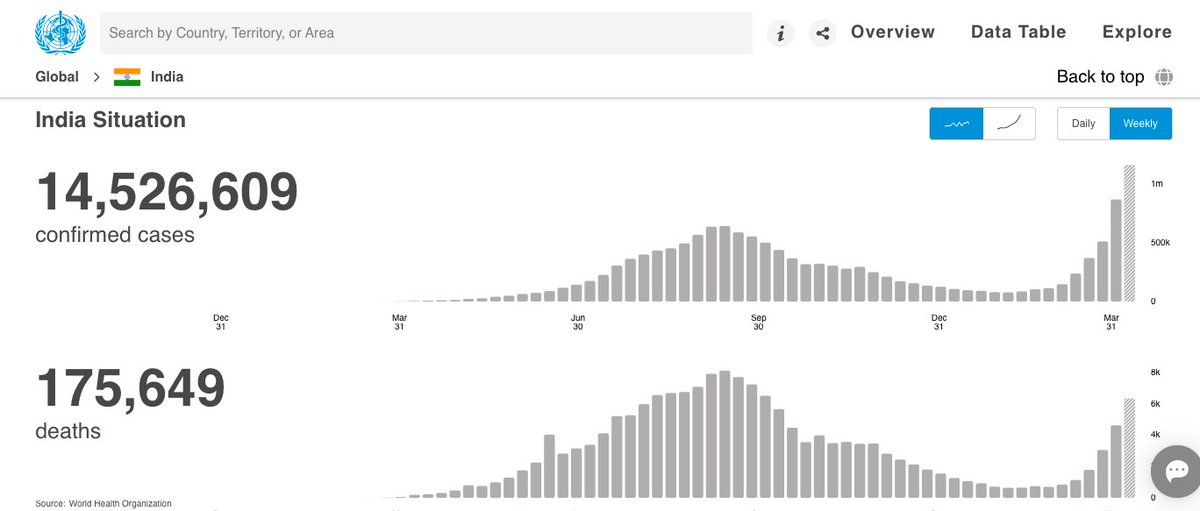
What do the RCTs conclude about #ConvalescentPlasma for #COVID_19? There were 10 trials, of which 3 were from India! Important that the second largest trial (464 patients) came from India, the PLACID trial by @ICMRDelhi. The largest was #RECOVERY (10406 patients) from the UK NHS
The PLACID trial, was in fact, the first large trial to be reported. 

PLACID showed no improvement with #ConvalescentPlasma with respect to its composite primary outcome of all cause mortality and progression to severe disease. Neither did it show any difference with biomarkers of severity of disease, or in neutralizing antibody titres



A meta analysis of the 10 RCTs was performed. This too did not show any difference between #ConvalescentPlasma and standard of care. However, physicians kept promoting, patients’ families kept demanding…



Thousands of patients families scoured around trying to find donors. Social media was rife with requests and pleas for #ConvalescentPlasma donations. Celebrities made fervent pleas to their followers and urged them to donate
We now have the results of the #RECOVERY trial – by far the largest trial ever done for #COVID_19 treatment. A phenomenal effort from the @NHSuk , @PeterHorby, @MartinLandray and colleagues

#RECOVERY recruited more than 11500 patients and compared between #ConvalescentPlasma and standard of care. Again, there was no difference in mortality. Basically, what this meant was that #ConvalescentPlasma DOES NOT WORK in #COVID_19



Not only in the whole set of patients, #ConvalescentPlasma did not work in ANY subset of patients.

And an updated meta analysis of 12 randomized trials confirms that #ConvalescentPlasma does not improve any mortality from #COVID_19

We have to let science decide our treatment policy. Not personal opinions, eminence, or experience. And based on very good science, we now know that #ConvalescentPlasma is not useful in #COVID_19
I repeat. #ConvalescentPlasma is not useful for the treatment of #COVID_19. The end.
• • •
Missing some Tweet in this thread? You can try to
force a refresh